Departments of Cutaneous Oncology and Immunology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, USA.
Evidence Synthesis and Decision Modeling, Precision HEOR, Vancouver, Canada.
ESMO Open. 2021 Apr;6(2):100050. doi: 10.1016/j.esmoop.2021.100050. Epub 2021 Feb 6.
Approved first-line treatments for patients with BRAF V600-mutant advanced melanoma include nivolumab (a programmed cell death protein 1 inhibitor) plus ipilimumab (a cytotoxic T lymphocyte antigen-4 inhibitor; NIVO+IPI) and the BRAF/MEK inhibitors dabrafenib plus trametinib (DAB+TRAM), encorafenib plus binimetinib (ENCO+BINI), and vemurafenib plus cobimetinib (VEM+COBI). Results from prospective randomized clinical trials (RCTs) comparing these treatments have not yet been reported. This analysis evaluated the relative efficacy and safety of NIVO+IPI versus DAB+TRAM, ENCO+BINI, and VEM+COBI in patients with BRAF-mutant advanced melanoma using a matching-adjusted indirect comparison (MAIC).
A systematic literature review identified RCTs for DAB+TRAM, ENCO+BINI, and VEM+COBI in patients with BRAF-mutant advanced melanoma. Individual patient-level data for NIVO+IPI were derived from the phase III CheckMate 067 trial (BRAF-mutant cohort) and restricted to match the inclusion/exclusion criteria of the comparator trials. Treatment effects for overall survival (OS) and progression-free survival (PFS) were estimated using Cox proportional hazards and time-varying hazard ratio (HR) models. Safety outcomes (grade 3 or 4 treatment-related adverse events) with NIVO+IPI and the comparators were compared.
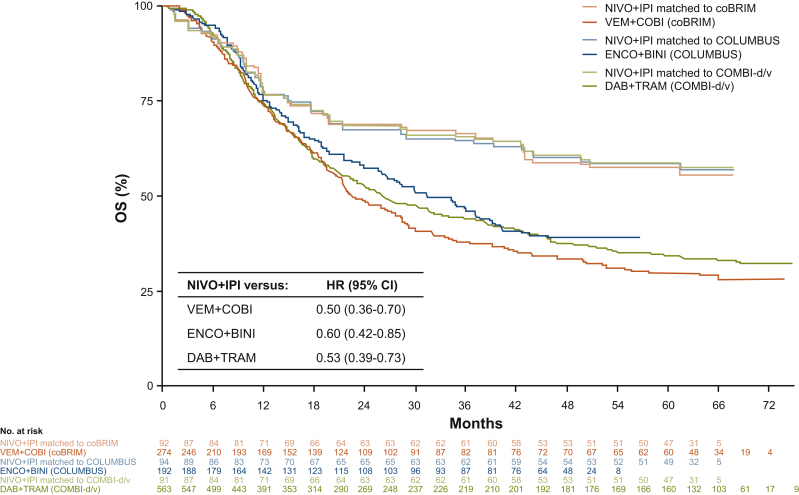
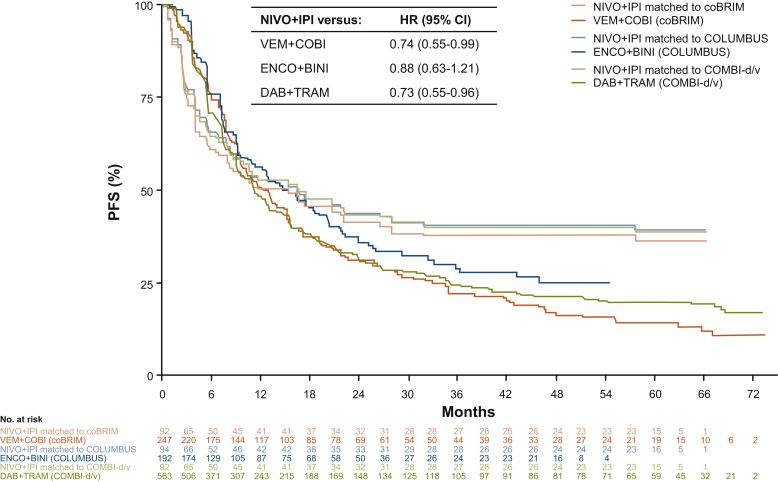
In the Cox proportional hazards analysis, NIVO+IPI showed improved OS compared with DAB+TRAM (HR = 0.53; 95% confidence interval [CI], 0.39-0.73), ENCO+BINI (HR = 0.60; CI, 0.42-0.85), and VEM+COBI (HR = 0.50; CI, 0.36-0.70) for the overall study period. In the time-varying analysis, NIVO+IPI was associated with significant improvements in OS and PFS compared with the BRAF/MEK inhibitors 12 months after treatment initiation. There were no significant differences between NIVO+IPI and BRAF/MEK inhibitor treatment from 0 to 12 months. Safety outcomes favored DAB+TRAM over NIVO+IPI, whereas NIVO+IPI was comparable to VEM+COBI.
Results of this MAIC demonstrated durable OS and PFS benefits for patients with BRAF-mutant advanced melanoma treated with NIVO+IPI compared with BRAF/MEK inhibitors, with the greatest benefits noted after 12 months.
批准的用于 BRAF V600 突变型晚期黑色素瘤患者的一线治疗方法包括纳武利尤单抗(一种程序性细胞死亡蛋白 1 抑制剂)加伊匹单抗(一种细胞毒性 T 淋巴细胞抗原 4 抑制剂;NIVO+IPI)和 BRAF/MEK 抑制剂达拉非尼加曲美替尼(DAB+TRAM)、恩考芬尼加比美替尼(ENCO+BINI)和维莫非尼加考比替尼(VEM+COBI)。尚未报告比较这些治疗方法的前瞻性随机临床试验(RCT)的结果。这项分析使用匹配调整间接比较(MAIC)评估了 NIVO+IPI 与 DAB+TRAM、ENCO+BINI 和 VEM+COBI 在 BRAF 突变型晚期黑色素瘤患者中的相对疗效和安全性。
系统文献检索确定了用于 BRAF 突变型晚期黑色素瘤患者的 DAB+TRAM、ENCO+BINI 和 VEM+COBI 的 RCT。纳武利尤单抗+伊匹单抗的个体患者水平数据来自 III 期 CheckMate 067 试验(BRAF 突变型队列),并限制为匹配比较试验的纳入/排除标准。使用 Cox 比例风险和时变风险比(HR)模型估计总生存期(OS)和无进展生存期(PFS)的治疗效果。比较了 NIVO+IPI 和比较药物的安全性结局(3 级或 4 级治疗相关不良事件)。
在 Cox 比例风险分析中,与 DAB+TRAM(HR=0.53;95%置信区间 [CI],0.39-0.73)、ENCO+BINI(HR=0.60;CI,0.42-0.85)和 VEM+COBI(HR=0.50;CI,0.36-0.70)相比,NIVO+IPI 显示出改善的 OS。在时变分析中,与 BRAF/MEK 抑制剂相比,NIVO+IPI 在治疗开始后 12 个月时与 OS 和 PFS 的显著改善相关。在 0 至 12 个月期间,NIVO+IPI 与 BRAF/MEK 抑制剂治疗之间没有显著差异。安全性结局有利于 DAB+TRAM 而非 NIVO+IPI,而 NIVO+IPI 与 VEM+COBI 相当。
这项 MAIC 的结果表明,与 BRAF/MEK 抑制剂相比,NIVO+IPI 治疗 BRAF 突变型晚期黑色素瘤患者具有持久的 OS 和 PFS 获益,在治疗后 12 个月时获益最大。