Pennington Biomedical Research Center, Baton Rouge, LA (C.H., J.L.D., C.K.M., R.L.N., J.W.A., C.A.M., K.D.D., E.F.M., W.D.J., D.Z., P.T.K.).
Department of Medicine and Feist-Weiller Cancer Center, Louisiana State University Health Sciences Center, Shreveport (C.L.A., T.C.D.).
Circulation. 2021 Mar 23;143(12):1202-1214. doi: 10.1161/CIRCULATIONAHA.120.051328. Epub 2021 Feb 9.
Intensive lifestyle interventions (ILIs) are the first-line approach to effectively treat obesity and manage associated cardiometabolic risk factors. Because few people have access to ILIs in academic health centers, primary care must implement similar approaches for a meaningful effect on obesity and cardiometabolic disease prevalence. To date, however, effective lifestyle-based obesity treatment in primary care is limited. We examined the effectiveness of a pragmatic ILI for weight loss delivered in primary care among a racially diverse, low-income population with obesity for improving cardiometabolic risk factors over 24 months.
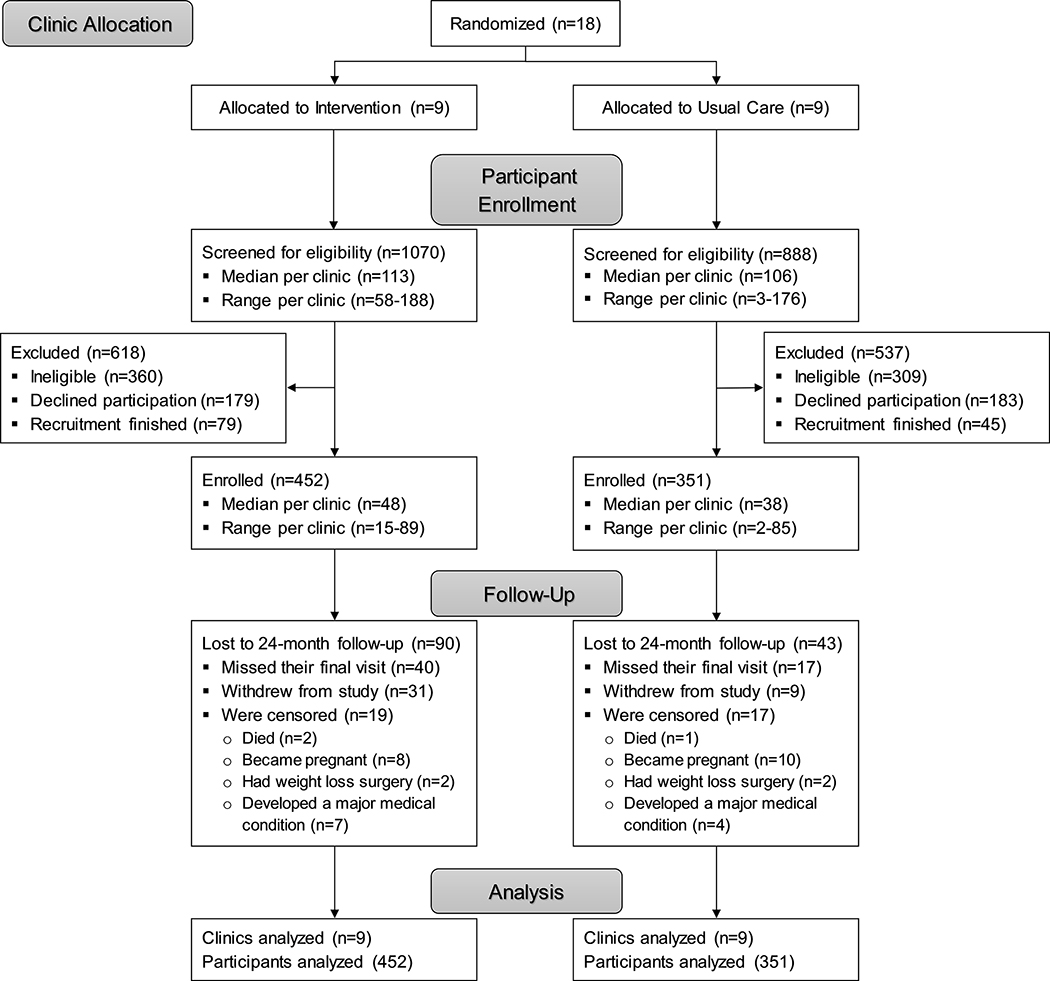
The PROPEL trial (Promoting Successful Weight Loss in Primary Care in Louisiana) randomly allocated 18 clinics equally to usual care or an ILI and subsequently enrolled 803 (351 usual care, 452 ILI) adults (67% Black, 84% female) with obesity from participating clinics. The usual care group continued to receive their normal primary care. The ILI group received a 24-month high-intensity lifestyle-based obesity treatment program, embedded in the clinic setting and delivered by health coaches in weekly sessions initially and monthly sessions in months 7 through 24.
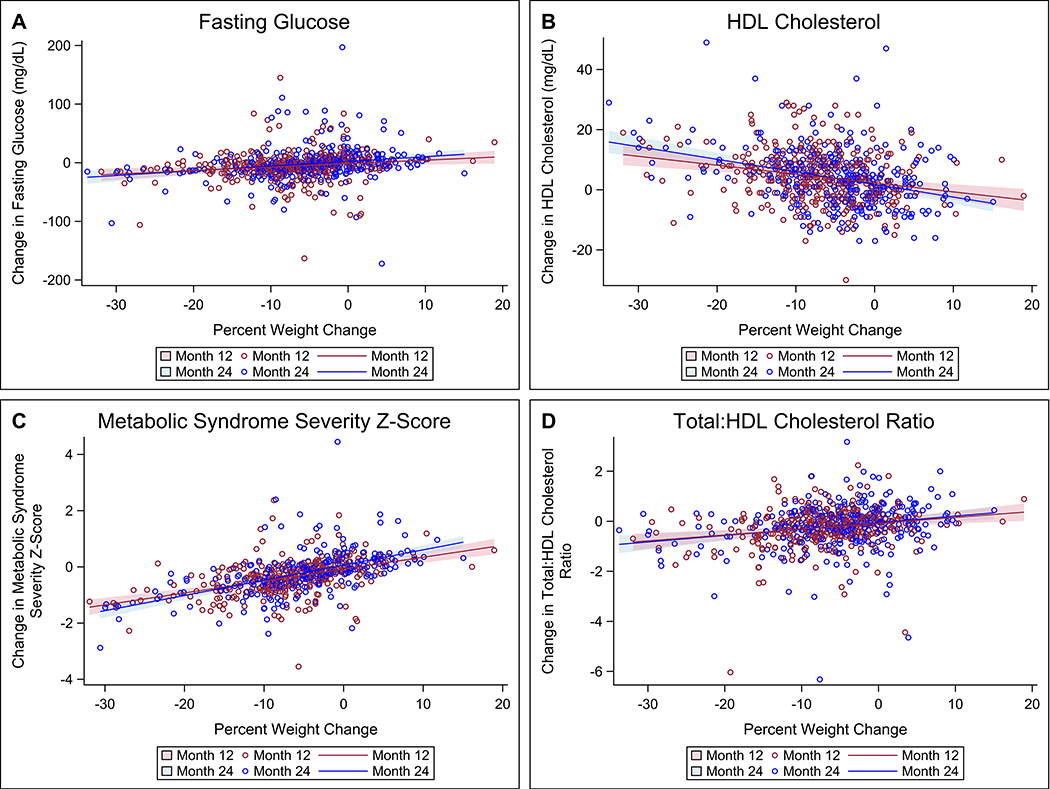
As recently demonstrated, participants receiving the PROPEL ILI lost significantly more weight over 24 months than those receiving usual care (mean difference, -4.51% [95% CI, -5.93 to -3.10]; <0.01). Fasting glucose decreased more in the ILI group compared with the usual care group at 12 months (mean difference, -7.1 mg/dL [95% CI, -12.0 to -2.1]; <0.01) but not 24 months (mean difference, -0.8 mg/dL [95% CI, -6.2 to 4.6]; =0.76). Increases in high-density lipoprotein cholesterol were greater in the ILI than in the usual care group at both time points (mean difference at 24 months, 4.6 mg/dL [95% CI, 2.9-6.3]; <0.01). Total:high-density lipoprotein cholesterol ratio and metabolic syndrome severity ( score) decreased more in the ILI group than in the usual care group at both time points, with significant mean differences of the change of -0.31 (95% CI, -0.47 to -0.14; <0.01) and -0.21 (95% CI, -0.36 to -0.06; =0.01) at 24 months, respectively. Changes in total cholesterol, low-density lipoprotein cholesterol, triglycerides, and blood pressure did not differ significantly between groups at any time point.
A pragmatic ILI consistent with national guidelines and delivered by trained health coaches in primary care produced clinically relevant improvements in cardiometabolic health in an underserved population over 24 months. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT02561221.
强化生活方式干预(ILI)是有效治疗肥胖症和管理相关心血管代谢风险因素的首选方法。由于在学术健康中心很少有人能够获得 ILI,初级保健必须实施类似的方法,才能对肥胖症和心血管代谢疾病的患病率产生有意义的影响。然而,迄今为止,初级保健中基于生活方式的有效肥胖症治疗方法有限。我们研究了在一个种族多样化、低收入的肥胖人群中,在初级保健中实施实用的 ILI 对减肥的有效性,以改善 24 个月时的心血管代谢风险因素。
PROPEL 试验(在路易斯安那州的初级保健中促进成功减肥)将 18 个诊所平均随机分配到常规护理或 ILI,随后从参与诊所招募了 803 名(常规护理 351 名,ILI 452 名)肥胖成年人(67%为黑人,84%为女性)。常规护理组继续接受他们的常规初级保健。ILI 组接受了为期 24 个月的高强度基于生活方式的肥胖症治疗方案,该方案嵌入在诊所环境中,并由健康教练在最初的每周一次和第 7 至 24 个月的每月一次的会议中提供。
正如最近所证明的,与接受常规护理的参与者相比,接受 PROPEL ILI 的参与者在 24 个月内体重减轻明显更多(平均差异,-4.51%[95%置信区间,-5.93 至-3.10];<0.01)。与常规护理组相比,ILI 组在 12 个月时空腹血糖下降更多(平均差异,-7.1mg/dL[95%置信区间,-12.0 至-2.1];<0.01),但在 24 个月时没有下降(平均差异,-0.8mg/dL[95%置信区间,-6.2 至 4.6];=0.76)。在 24 个月时,高密度脂蛋白胆固醇的增加在 ILI 组中比在常规护理组中更为显著(平均差异,4.6mg/dL[95%置信区间,2.9-6.3];<0.01)。在 24 个月时,总胆固醇:高密度脂蛋白胆固醇比值和代谢综合征严重程度(评分)在 ILI 组中比在常规护理组中下降更多,变化的平均差异有统计学意义,分别为-0.31(95%置信区间,-0.47 至-0.14;<0.01)和-0.21(95%置信区间,-0.36 至-0.06;=0.01)。在任何时间点,两组之间的总胆固醇、低密度脂蛋白胆固醇、甘油三酯和血压的变化均无显著差异。
符合国家指南的实用 ILI,并由经过培训的健康教练在初级保健中提供,在 24 个月内为服务不足的人群提供了心血管代谢健康方面的临床相关改善。注册:网址:https://www.clinicaltrials.gov;唯一标识符:NCT02561221。