IgangaMayuge Health and Demographic Surveillance System, Makerere University Centre for Health and Population Research, Iganga, Uganda.
Kintampo Health Research Centre, Kintampo, Ghana.
Popul Health Metr. 2021 Feb 8;19(Suppl 1):7. doi: 10.1186/s12963-020-00232-1.
Global mortality estimates remain heavily dependent on household surveys in low- and middle-income countries, where most under-five deaths occur. Few studies have assessed the accuracy of mortality data or determinants of capturing births in surveys.
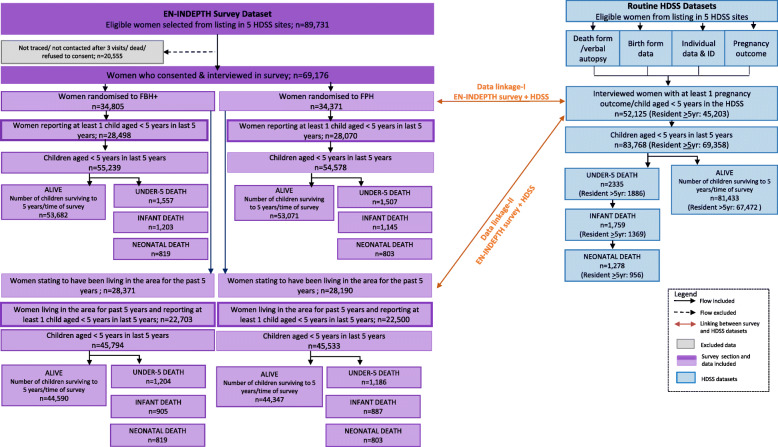
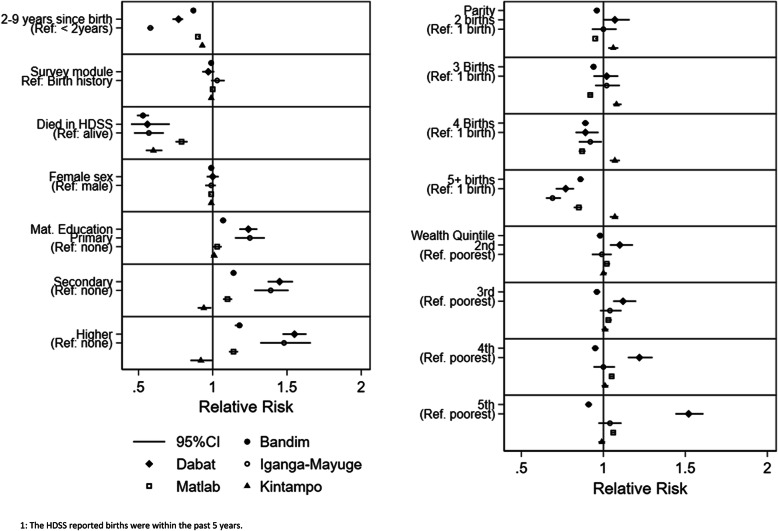
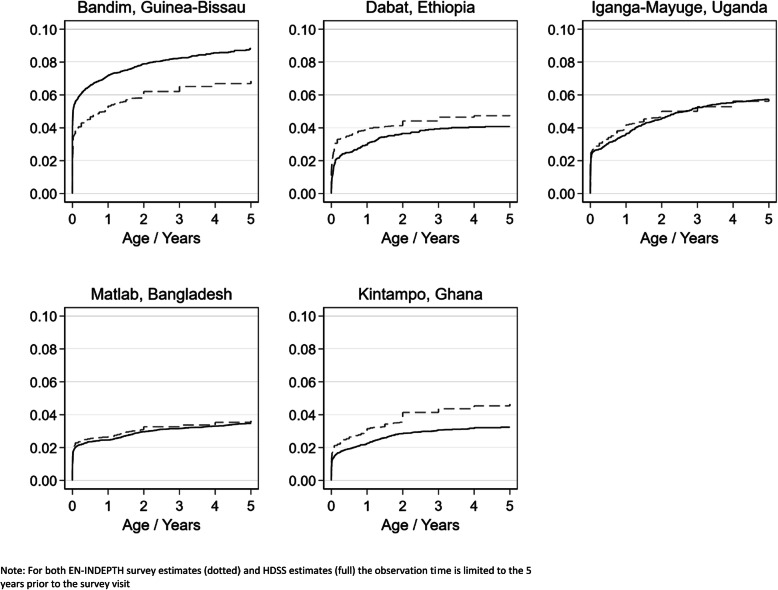
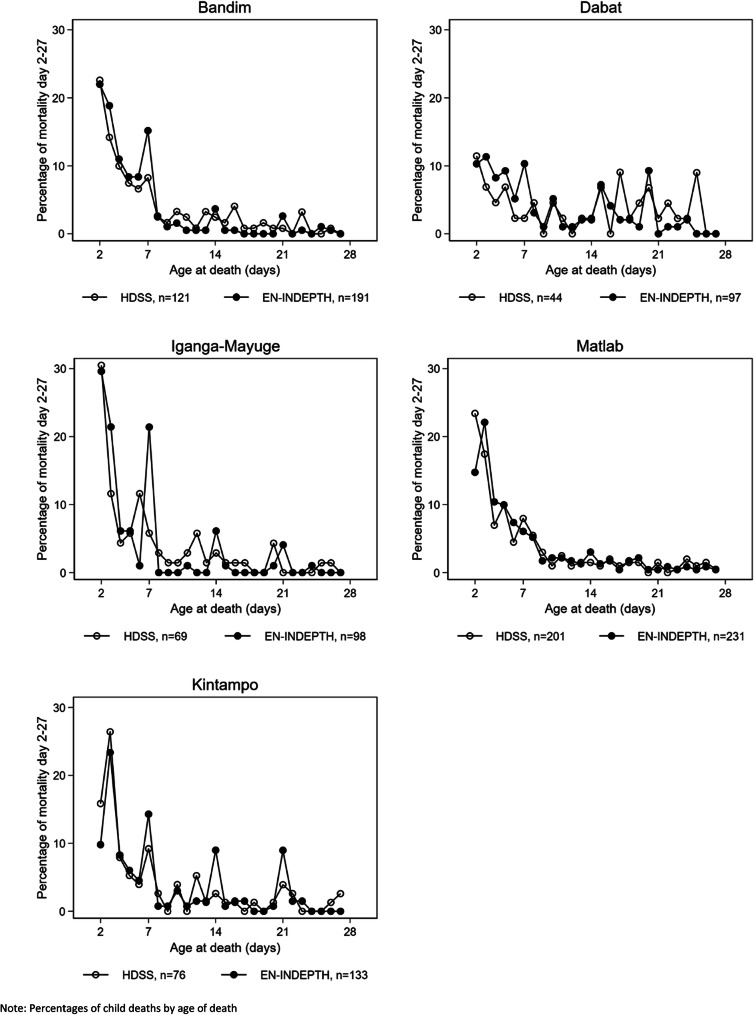
The Every Newborn-INDEPTH study (EN-INDEPTH) included a large, multi-country survey of women aged 15-49 interviewed about livebirths and their survival status in five Health and Demographic Surveillance Systems (HDSSs). The HDSSs undertake regular household visits to register births and deaths for a given population. We analysed EN-INDEPTH survey data to assess background factors associated with not recalling a complete date-of-birth. We calculated Kaplan-Meier survival estimates for both survey and HDSS data and describe age-at-death distributions during the past 5 years for children born to the same women. We assessed the proportion of HDSS-births that could be matched on month-of-birth to survey-births and used regression models to identify factors associated with matching.
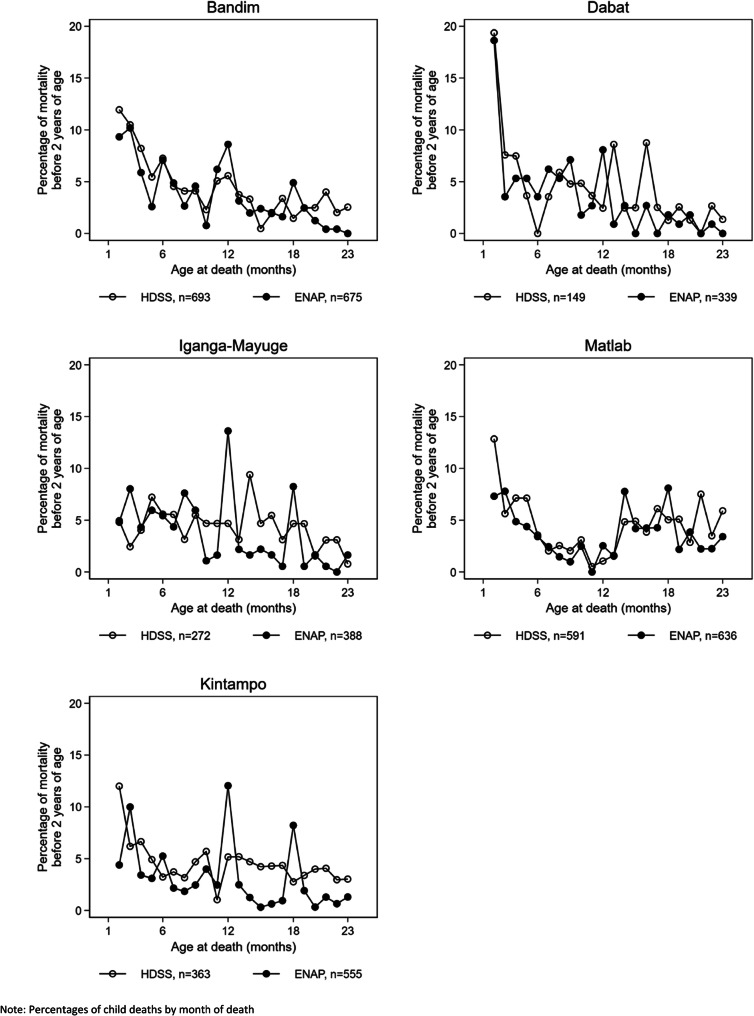
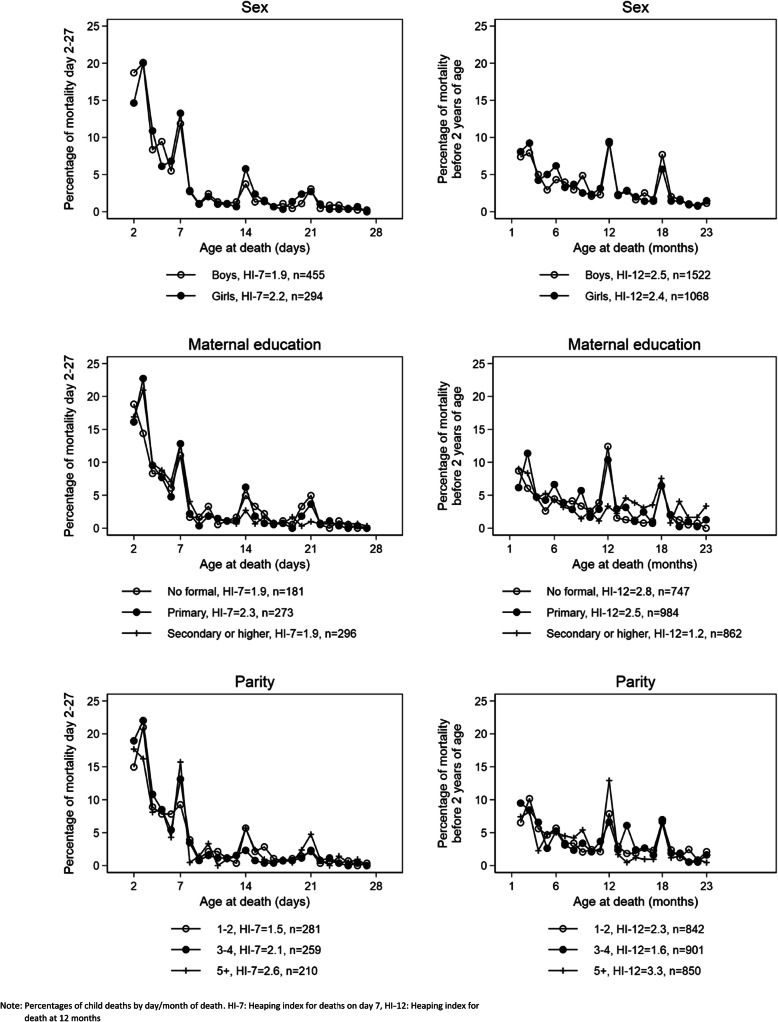
69,176 women interviewed in the survey reported 109,817 births and 3064 deaths in children under 5 years in the 5 years prior to the survey. In the HDSS data, the same women had 83,768 registered births and 2335 under-five deaths in the same period. A complete date-of-birth was not reported for 1-7% of survey-births. Birthdates were less likely to be complete for dead children and children born to women of higher parity or with little/no education. Distributions of reported age-at-death indicated heaping at full weeks (neonatal period) and at 12 months. Heaping was more pronounced in the survey data. Survey estimates of under-five mortality rates were similar to HDSS estimates of under-five mortality in two of five sites, higher in the survey in two sites (15%, 41%) and lower (24%) in one site. The proportion of HDSS-births matched to survey-births ranged from 51 to 89% across HDSSs and births of children who had died were less likely to be matched.
Mortality estimates in the survey and HDSS were not markedly different for most sites. However, neither source is a "gold standard" and both sources miss some events. Research is required to improve capture and accuracy to better track newborn and child survival targets.
全球死亡率估计仍然严重依赖于中低收入国家的家庭调查,而这些国家是大多数五岁以下儿童死亡的发生地。很少有研究评估死亡率数据的准确性或调查中捕捉出生的决定因素。
Every Newborn-INDEPTH 研究(EN-INDEPTH)包括对五个健康和人口监测系统(HDSS)中 15-49 岁的妇女进行的一项大型多国调查,这些妇女接受了关于活产及其生存状况的访谈。HDSS 定期对家庭进行家访,为特定人群登记出生和死亡情况。我们分析了 EN-INDEPTH 调查数据,以评估与不完全回忆出生日期相关的背景因素。我们计算了调查和 HDSS 数据的 Kaplan-Meier 生存估计,并描述了过去 5 年中同一批妇女所生孩子的死亡年龄分布。我们评估了可以根据出生月份与调查出生相匹配的 HDSS 出生比例,并使用回归模型确定与匹配相关的因素。
在调查中接受访谈的 69176 名妇女报告了在调查前 5 年中 109817 名 5 岁以下儿童的 3064 例死亡。在 HDSS 数据中,同一批妇女在此期间登记了 83768 例出生和 2335 例 5 岁以下儿童死亡。调查中 1-7%的出生没有完整的出生日期。死产儿和多产或受教育程度低或无教育的妇女所生孩子的出生日期更不可能完整。报告的死亡年龄分布表明,在完整周(新生儿期)和 12 个月时存在堆积。在调查数据中,堆积现象更为明显。在五个地点中的两个地点,调查估计的五岁以下儿童死亡率与 HDSS 估计的五岁以下儿童死亡率相似,在两个地点(15%,41%)较高,在一个地点(24%)较低。在 HDSS 中,HDSS 出生与调查出生相匹配的比例从 51%到 89%不等,而且死亡儿童的出生更不可能匹配。
对于大多数地点,调查和 HDSS 的死亡率估计值没有明显差异。然而,这两种来源都不是“黄金标准”,并且都遗漏了一些事件。需要研究来提高捕获和准确性,以更好地跟踪新生儿和儿童的生存目标。