Keykhaei Mohammad, Masinaei Masood, Mohammadi Esmaeil, Azadnajafabad Sina, Rezaei Negar, Saeedi Moghaddam Sahar, Rezaei Nazila, Nasserinejad Maryam, Abbasi-Kangevari Mohsen, Malekpour Mohammad-Reza, Ghamari Seyyed-Hadi, Haghshenas Rosa, Koliji Kamyar, Kompani Farzad, Farzadfar Farshad
Non-Communicable Diseases Research Center, Endocrinology and Metabolism Population Sciences Institute, Tehran University of Medical Sciences, Tehran, Iran.
Department of Epidemiology and Biostatistics, Tehran University of Medical Sciences, Tehran, Iran.
Exp Hematol Oncol. 2021 Feb 8;10(1):11. doi: 10.1186/s40164-021-00198-2.
Hematologic malignancies (HMs) are a heterogeneous group of cancers that comprise diverse subgroups of neoplasms. So far, despite the major epidemiologic concerns about the quality of care, limited data are available for patients with HMs. Thus, we created a novel measure-Quality of Care Index (QCI)-to appraise the quality of care in different populations.
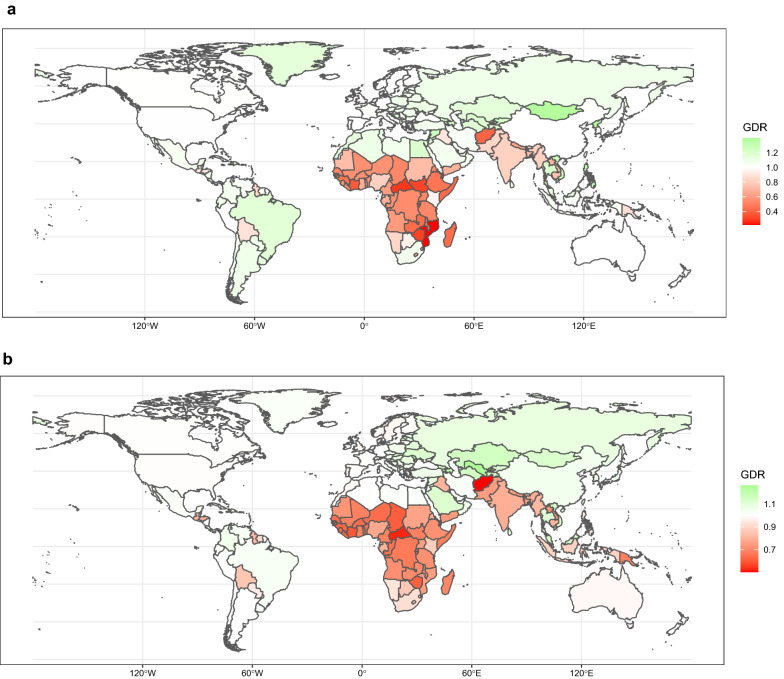
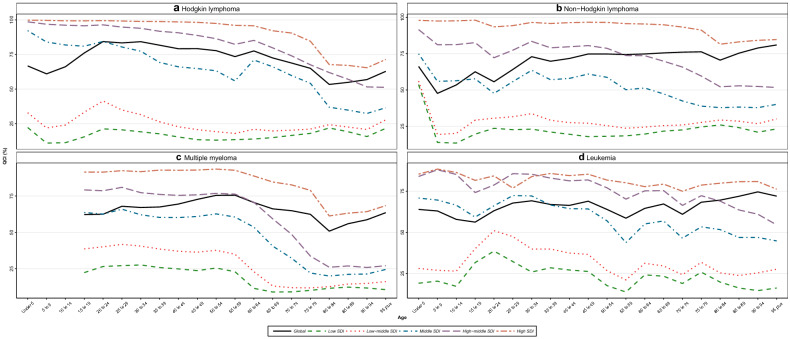
The Global Burden of Disease data from 1990 to 2017 applied in our study. We performed a principal component analysis on several secondary indices from the major primary indices, including incidence, prevalence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years (DALYs) to create the QCI, which provides an overall score of 0-100 of the quality of cancer care. We estimated the QCI for each age group on different scales and constructed the gender disparity ratio to evaluate the gender disparity of care in HMs.
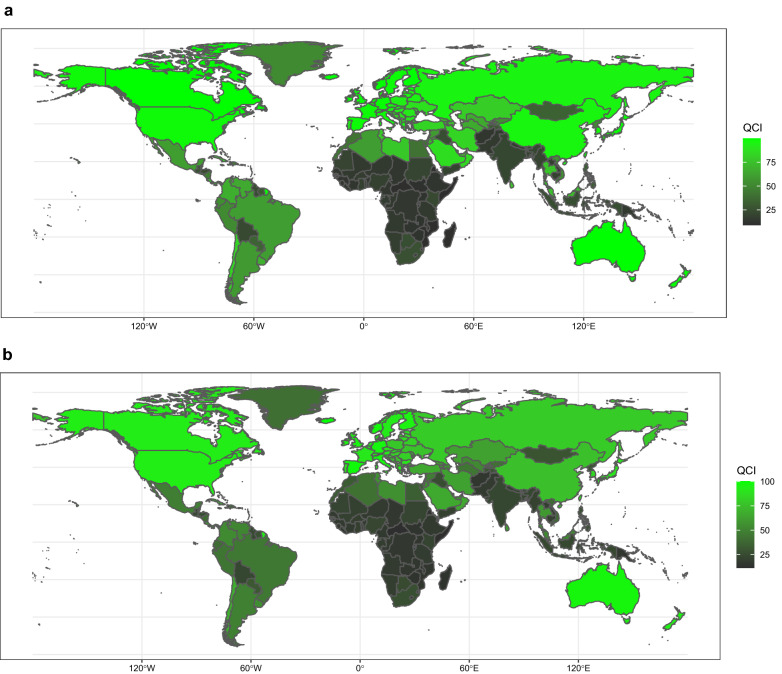
Globally, while the overall age-standardized incidence rate of HMs increased from 1990 to 2017, the age-standardized DALYs and death rates decreased during the same period. Across countries, in 2017, Iceland (100), New Zealand (100), Australia (99.9), and China (99.3) had the highest QCI scores for non-Hodgkin lymphoma, multiple myeloma, Hodgkin lymphoma, and leukemia. Conversely, Central African Republic (11.5 and 6.1), Eritrea (9.6), and Mongolia (5.4) had the lowest QCI scores for the mentioned malignancies respectively. Overall, the QCI score was positively associated with higher sociodemographic of nations, and was negatively associated with age advancing.
The QCI provides a robust metric to evaluate the quality of care that empowers policymakers on their responsibility to allocate the resources effectively. We found that there is an association between development status and QCI and gender equity, indicating that instant policy attention is demanded to improve health-care access.
血液系统恶性肿瘤(HMs)是一组异质性癌症,由多种肿瘤亚组组成。到目前为止,尽管对医疗质量存在重大流行病学担忧,但关于血液系统恶性肿瘤患者的数据有限。因此,我们创建了一种新的衡量指标——医疗质量指数(QCI),以评估不同人群的医疗质量。
我们的研究应用了1990年至2017年的全球疾病负担数据。我们对主要初级指标的几个次级指标进行了主成分分析,包括发病率、患病率、死亡率、寿命损失年数、残疾存活年数和残疾调整生命年(DALYs),以创建QCI,该指数提供了癌症医疗质量的0至100的总体评分。我们在不同尺度上估计了每个年龄组的QCI,并构建了性别差异比率以评估血液系统恶性肿瘤中医疗的性别差异。
在全球范围内,虽然1990年至2017年血液系统恶性肿瘤的总体年龄标准化发病率有所上升,但同期年龄标准化DALYs和死亡率有所下降。在各个国家中,2017年,冰岛(100)、新西兰(100)、澳大利亚(99.9)和中国(99.3)在非霍奇金淋巴瘤、多发性骨髓瘤、霍奇金淋巴瘤和白血病方面的QCI得分最高。相反,中非共和国(11.5和6.1)、厄立特里亚(9.6)和蒙古(5.4)在上述恶性肿瘤方面的QCI得分分别最低。总体而言,QCI得分与国家较高的社会人口统计学特征呈正相关,与年龄增长呈负相关。
QCI提供了一个强有力的指标来评估医疗质量,使政策制定者能够有效履行其分配资源的责任。我们发现发展状况与QCI和性别平等之间存在关联,这表明需要立即给予政策关注以改善医疗服务的可及性。