Non-Communicable Diseases Research Center, Endocrinology and Metabolism Population Sciences Institute, Tehran University of Medical Sciences, Tehran, Iran.
Cochrane Iran Associate Centre, National Institute for Medical Research Development (NIMAD), Tehran, Iran.
BMC Oral Health. 2021 Nov 2;21(1):558. doi: 10.1186/s12903-021-01918-0.
To measure the quality of care for lip and oral cavity cancer worldwide using the data from the Global Burden of Disease (GBD) Study 2017.
After devising four main indices of quality of care for lip and oral cavity cancer using GBD 2017 study's measures, including prevalence, incidence, years of life lost, years lived with disability, and disability-adjusted life years, we utilised principal component analysis (PCA) to determine a component that bears the most proportion of info among the others. This component of the PCA was considered as the Quality-of-Care Index (QCI) for lip and oral cavity cancer. The QCI score was then reported in both men and women worldwide and different countries based on the socio-demographic index (SDI) and World Bank classifications.
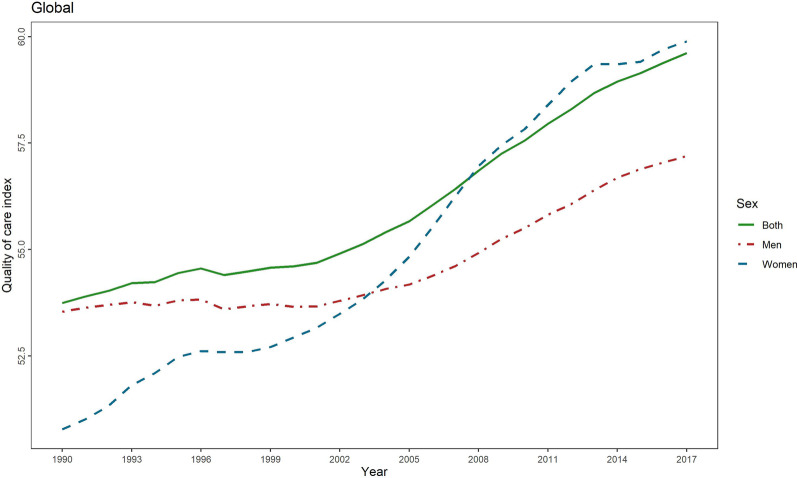
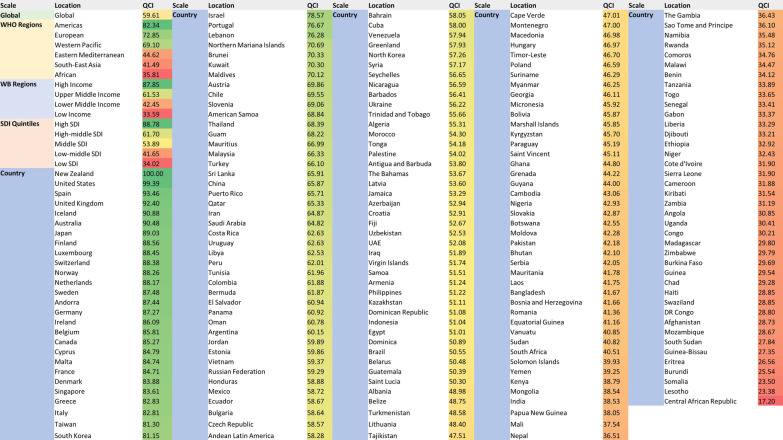
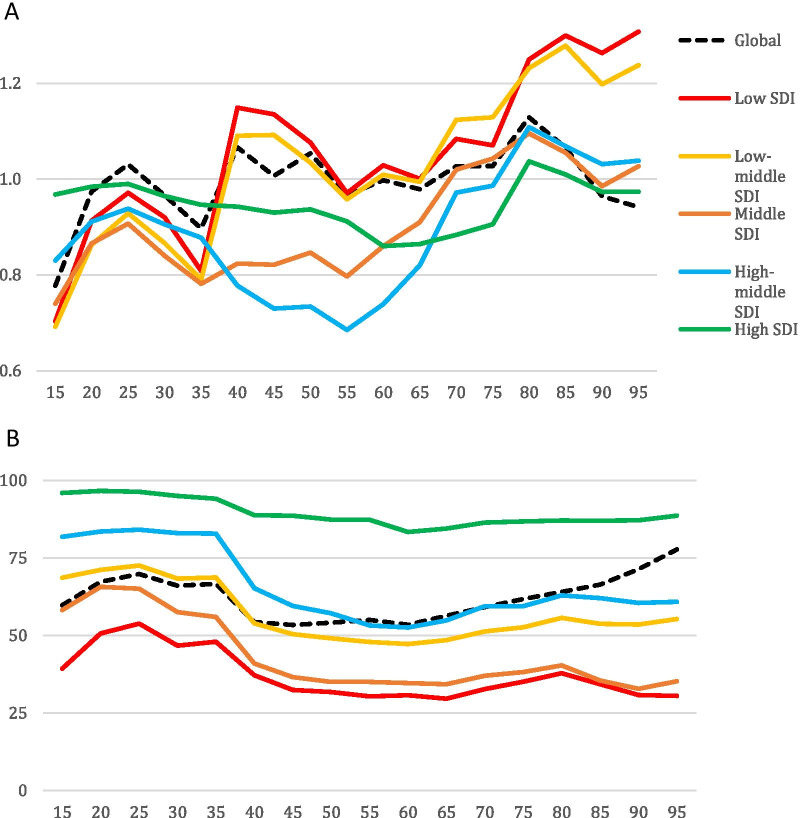
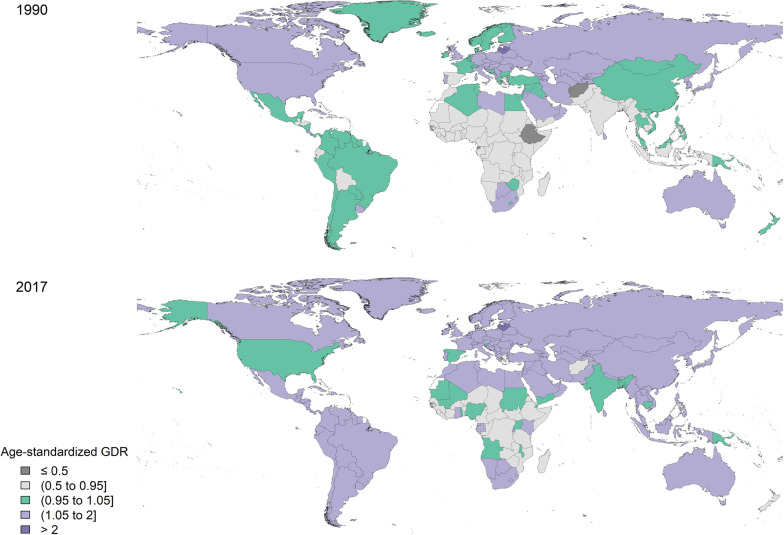
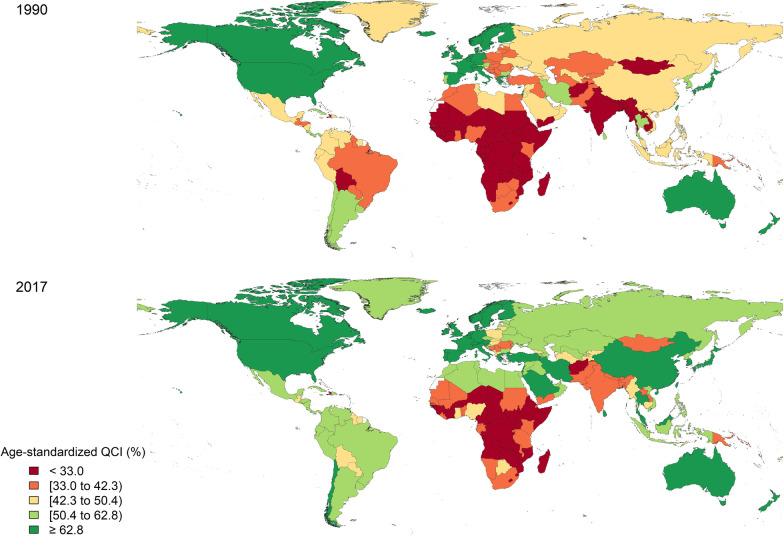
Between 1990 and 2017, care quality continuously increased globally (from 53.7 to 59.6). In 1990, QCI was higher for men (53.5 for men compared with 50.8 for women), and in 2017 QCI increased for both men and women, albeit a slightly higher rise for women (57.2 for men compared with 59.9 for women). During the same period, age-standardised QCI for lip and oral cavity cancer increased in all regions (classified by SDI and World Bank). Globally, the highest QCI scores were observed in the elderly age group, whereas the least were in the adult age group. Five countries with the least amount of QCIs were all African. In contrast, North American countries, West European countries and Australia had the highest indices.
The quality of care for lip and oral cavity cancer showed a rise from 1990 to 2017, a promising outcome that supports patient-oriented and preventive treatment policies previously advised in the literature. However, not all countries enjoyed such an increase in the QCI to the same extent. This alarming finding could imply a necessary need for better access to high-quality treatments for lip and oral cavity cancer, especially in central African countries and Afghanistan. More policies with a preventive approach and paying more heed to the early diagnosis, broad insurance coverage, and effective screening programs are recommended worldwide. More focus should also be given to the adulthood age group as they had the least QCI scores globally.
利用全球疾病负担(GBD)研究 2017 年的数据,衡量全球唇口腔癌的护理质量。
使用 GBD 2017 研究的措施设计唇口腔癌护理质量的四个主要指标,包括患病率、发病率、丧失的生命年、失能生命年和残疾调整生命年,我们利用主成分分析(PCA)确定在其他指标中承载最多信息的一个成分。该 PCA 成分被视为唇口腔癌的护理质量指数(QCI)。然后根据社会人口指数(SDI)和世界银行分类,在全球范围内以及不同国家报告男性和女性的 QCI 评分。
1990 年至 2017 年期间,全球护理质量持续提高(从 53.7 提高到 59.6)。1990 年,男性的 QCI 更高(男性为 53.5,女性为 50.8),而 2017 年男性和女性的 QCI 均有所提高,尽管女性的增幅略高(男性为 57.2,女性为 59.9)。在此期间,所有地区(按 SDI 和世界银行分类)的唇口腔癌年龄标准化 QCI 均有所增加。全球范围内,最高的 QCI 评分出现在老年组,而最低的出现在成年组。QCI 评分最低的五个国家都是非洲国家。相比之下,北美国家、西欧国家和澳大利亚的指数最高。
1990 年至 2017 年,唇口腔癌的护理质量有所提高,这是一个令人鼓舞的结果,支持文献中建议的以患者为导向和预防治疗政策。然而,并非所有国家的 QCI 都以同样的程度增加。这一令人担忧的发现可能意味着需要更好地获得高质量的唇口腔癌治疗,特别是在中非国家和阿富汗。建议全球范围内采取更多具有预防作用的政策,并更加关注早期诊断、广泛的保险覆盖范围和有效的筛查计划。还应更加关注成年年龄组,因为他们在全球范围内的 QCI 评分最低。