Department of Neurology, UMC Utrecht Brain Center, University Medical Center Utrecht, Utrecht, the Netherlands.
Department of Neurology, Erasmus MC - University Medical Center, Rotterdam, the Netherlands.
Diabetologia. 2021 Jun;64(6):1235-1245. doi: 10.1007/s00125-021-05393-8. Epub 2021 Feb 9.
AIMS/HYPOTHESIS: Type 2 diabetes, particularly with concomitant CVD, is associated with an increased risk of cognitive impairment. We assessed the effect on accelerated cognitive decline (ACD) of the DPP-4 inhibitor linagliptin vs the sulfonylurea glimepiride in individuals with type 2 diabetes.
The CAROLINA-COGNITION study was part of the randomised, double-blind, active-controlled CAROLINA trial that evaluated the cardiovascular safety of linagliptin vs glimepiride in individuals with age ≥40 and ≤85 years and HbA 48-69 mmol/mol (6.5-8.5%) receiving standard care, excluding insulin therapy. Participants were randomised 1:1 using an interactive telephone- and web-based system and treatment assignment was determined by a computer-generated random sequence with stratification by center. The primary cognitive outcome was occurrence of ACD at end of follow-up, defined as a regression-based index score ≤16th percentile on either the Mini-Mental State Examination (MMSE) or a composite measure of attention and executive functioning, in participants with a baseline MMSE score ≥24. Prespecified additional analyses included effects on ACD at week 160, in subgroups (sex, age, race, ethnicity, depressive symptoms, cardiovascular risk, duration of type 2 diabetes, albuminuria), and absolute changes in cognitive performance. Participants, caregivers, and people involved in measurements, examinations or adjudication, were all masked to treatment assignment.
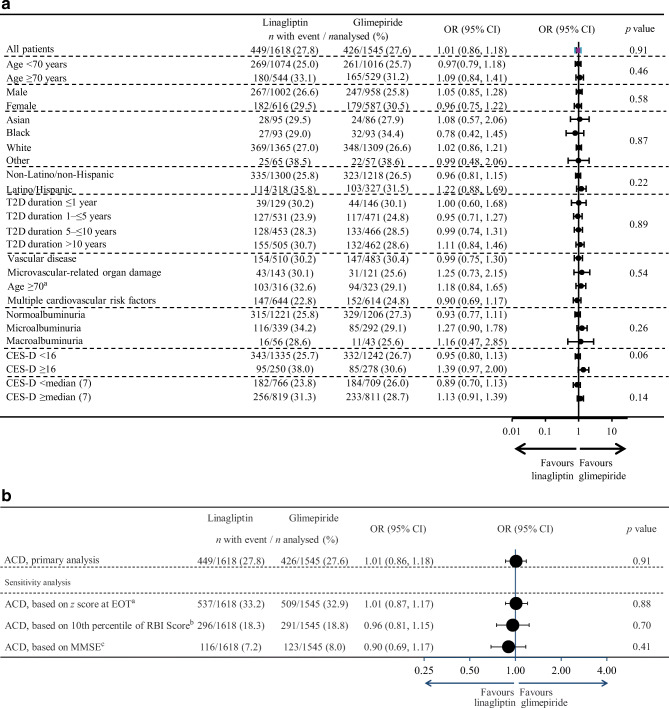
Of 6033 participants recruited from hospital and primary care sites, 3163 (38.0% female, mean age/diabetes duration 64/7.6 years, MMSE score 28.5, HbA 54 mmol/mol [7.1%]) represent the CAROLINA-COGNITION cohort. Over median 6.1 years, ACD occurred in 27.8% (449/1618, linagliptin) vs 27.6% (426/1545, glimepiride), OR 1.01 (95% CI 0.86, 1.18). Also, no differences in ACD were observed at week 160 (OR 1.07 [0.91, 1.25]), between treatments across subgroups, or for absolute cognitive changes.
CONCLUSIONS/INTERPRETATION: In a large, international outcome trial in people with relatively early type 2 diabetes at elevated cardiovascular risk, no difference in risk for ACD was observed between linagliptin and glimepiride over 6.1 years.
This study was sponsored by Boehringer Ingelheim.
ClinicalTrials.gov NCT01243424.
目的/假设:2 型糖尿病,尤其是伴有心血管疾病(CVD)的 2 型糖尿病,与认知障碍风险增加相关。我们评估了二肽基肽酶-4 抑制剂利格列汀与磺酰脲类药物格列美脲对 2 型糖尿病患者加速认知衰退(ACD)的影响。
CAROLINA-COGNITION 研究是一项随机、双盲、活性对照的 CAROLINA 试验的一部分,该试验评估了利格列汀与格列美脲在年龄≥40 岁且≤85 岁、HbA 48-69mmol/mol(6.5-8.5%)且接受标准治疗(不包括胰岛素治疗)的患者中的心血管安全性。参与者使用交互式电话和网络系统以 1:1 的比例随机分组,治疗分配由计算机生成的随机序列确定,并按中心进行分层。主要认知结局是在随访结束时发生 ACD,定义为基线 MMSE 评分≥24 的参与者中基于回归的指数评分≤第 16 百分位数,或注意力和执行功能综合测量中的评分≤第 16 百分位数。预先规定的其他分析包括在第 160 周时对 ACD 的影响、亚组(性别、年龄、种族、民族、抑郁症状、心血管风险、2 型糖尿病病程、白蛋白尿)以及认知表现的绝对变化。参与者、护理人员以及参与测量、检查或裁决的人员均对治疗分配不知情。
在从医院和初级保健机构招募的 6033 名参与者中,3163 名(38.0%女性,平均年龄/糖尿病病程 64/7.6 岁,MMSE 评分为 28.5,HbA 54mmol/mol[7.1%])代表了 CAROLINA-COGNITION 队列。中位 6.1 年期间,ACD 发生率为 27.8%(449/1618,利格列汀)vs 27.6%(426/1545,格列美脲),OR 1.01(95%CI 0.86,1.18)。此外,在第 160 周时,两种治疗方法之间(OR 1.07[0.91,1.25])、在各亚组之间(OR 1.07[0.91,1.25])以及在认知绝对变化方面,均未观察到 ACD 的差异。
结论/解释:在一项针对心血管风险较高的 2 型糖尿病患者的大型国际结局试验中,6.1 年内,利格列汀与格列美脲在 ACD 风险方面无差异。
本研究由勃林格殷格翰公司赞助。
ClinicalTrials.gov NCT01243424。