Department of Clinical Therapeutics, Alexandra General Hospital, National and Kapodistrian University of Athens School of Medicine, Athens, Greece.
Harvard Medical School, Boston, MA.
Blood Adv. 2021 Feb 9;5(3):725-736. doi: 10.1182/bloodadvances.2020002378.
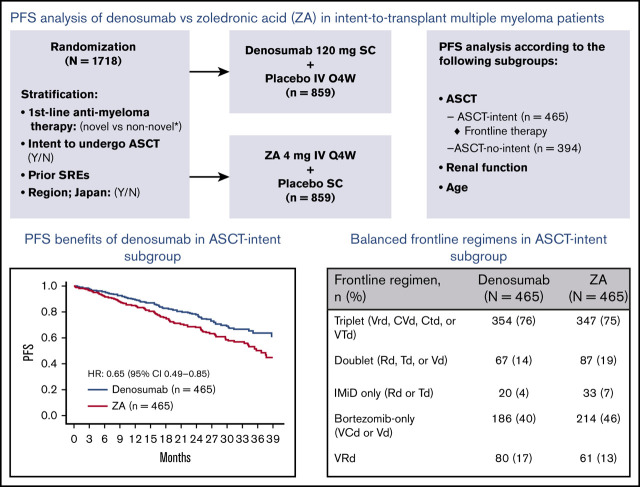
An exploratory end point from a recent trial in patients with newly diagnosed multiple myeloma showed that median progression-free survival (PFS) was increased by 10.7 months with denosumab vs zoledronic acid. We performed additional analyses to identify factors that may have contributed to the favorable PFS with denosumab. Ad hoc analyses were performed for patients intending to undergo autologous stem cell transplantation (ASCT; ASCT intent), not intending to undergo ASCT (ASCT no intent), and intent-to-treat according to age (<70 or ≥70 years) and baseline renal function (≤60 mL/min or >60 mL/min creatinine clearance [CrCl]). Of 1718 patients, 930 (54.1%) were in the ASCT-intent subgroup, and 788 (45.9%) were in the ASCT-no-intent subgroup. In the ASCT-intent subgroup, frontline triplet (median PFS, not estimable vs 35.7 months; hazard ratio [HR] [95% confidence interval (CI)], 0.65 [0.47-0.90]; descriptive P = .009) or bortezomib-only (median PFS, not estimable vs not estimable; HR [95% CI], 0.61 [0.39-0.95]; descriptive P = .029) induction regimens demonstrated the strongest PFS benefit favoring denosumab vs zoledronic acid. In the ASCT-no-intent subgroup, no benefit with denosumab vs zoledronic acid was observed. PFS favored denosumab vs zoledronic acid in patients with CrCl >60 mL/min and in patients <70 years old, but no difference was observed in patients with CrCl ≤60 mL/min or patients ≥70 years old. The PFS difference observed with denosumab is one of the notable benefits reported in newly diagnosed multiple myeloma and was most pronounced in patients intending to undergo ASCT and those who received proteasome inhibitor (PI)-based triplet regimens. This study was registered at www.clinicaltrials.gov as #NCT01345019.
一项近期针对初诊多发性骨髓瘤患者的探索性终点研究显示,与唑来膦酸相比,地舒单抗可使无进展生存期(PFS)延长 10.7 个月。我们进行了额外的分析,以确定可能导致地舒单抗 PFS 获益的因素。对有意愿行自体造血干细胞移植(ASCT;ASCT 意向)、无意愿行 ASCT(ASCT 无意愿)以及按年龄(<70 岁或≥70 岁)和基线肾功能(≤60mL/min 或>60mL/min 肌酐清除率[CrCl])意向治疗患者进行了特定分析。在 1718 例患者中,930 例(54.1%)为 ASCT 意向亚组,788 例(45.9%)为 ASCT 无意愿亚组。在 ASCT 意向亚组中,一线三联方案(中位 PFS,不可评估 vs 35.7 个月;风险比[HR] [95%置信区间(CI)],0.65 [0.47-0.90];描述性 P =.009)或硼替佐米单药(中位 PFS,不可评估 vs 不可评估;HR [95%CI],0.61 [0.39-0.95];描述性 P =.029)诱导方案对地舒单抗较唑来膦酸显示出最强的 PFS 获益。在 ASCT 无意愿亚组中,地舒单抗与唑来膦酸相比无获益。在 CrCl>60mL/min 和年龄<70 岁的患者中,地舒单抗 PFS 获益优于唑来膦酸,但在 CrCl≤60mL/min 或年龄≥70 岁的患者中,两者无差异。与唑来膦酸相比,地舒单抗观察到的 PFS 差异是初诊多发性骨髓瘤的显著获益之一,在有 ASCT 意向的患者和接受蛋白酶体抑制剂(PI)三联方案的患者中最为显著。本研究在 www.clinicaltrials.gov 注册,编号为#NCT01345019。