Martínez-Castelao Alberto, Soler María José, Górriz Teruel José Luis, Navarro-González Juan F, Fernandez-Fernandez Beatriz, de Alvaro Moreno Fernando, Ortiz Alberto
Nephrology department, Bellvitge University Hospital, Barcelona, Spain.
GEENDIAB (Grupo Español de Estudio de la Nefropatía Diabética), Sociedad Española Nefrología (SEN), Santander, Spain.
Clin Kidney J. 2020 Aug 5;14(1):5-8. doi: 10.1093/ckj/sfaa125. eCollection 2021 Jan.
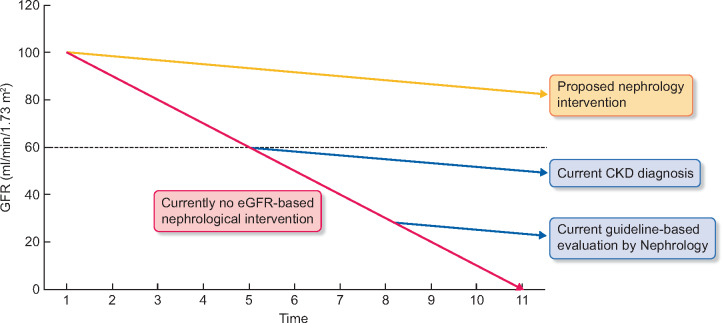
Age-standardized rates of diabetes mellitus (DM)-related complications, such as acute myocardial infarction, stroke or amputations, have decreased in recent years, but this was not associated with a clear reduction of the incidence of advanced chronic kidney disease (CKD) requiring renal replacement therapy. The early detection of diabetic kidney disease (DKD) is a key to reduce complications, morbidity and mortality. Consensus documents and clinical practice guidelines recommend referral of DM patients to nephrology when the estimated glomerular filtration rate falls below 30 mL/min/1.73 m or when albuminuria exceeds 300 mg/g urinary creatinine. Conceptually, it strikes as odd that patients with CKD are referred to the specialist caring for the prevention and treatment of CKD only when >70% of the functioning kidney mass has been lost. The increasing global health burden of CKD, driven in large part by DKD, the suboptimal impact of routine care on DKD outcomes as compared with other DM complications, the realization that successful therapy of CKD requires early diagnosis and intervention, the advances in earlier diagnosis of kidney injury and the recent availability of antidiabetic drugs with a renal mechanism of action and lack of hypoglycaemia risk, which additionally are cardio- and nephroprotective, all point towards a paradigm shift in the care for DM patients in which they should be referred earlier to nephrology as part of a coordinated and integrated care approach.
近年来,糖尿病(DM)相关并发症(如急性心肌梗死、中风或截肢)的年龄标准化发病率有所下降,但这与需要肾脏替代治疗的晚期慢性肾脏病(CKD)发病率的明显降低并无关联。糖尿病肾病(DKD)的早期检测是降低并发症、发病率和死亡率的关键。共识文件和临床实践指南建议,当估计肾小球滤过率低于30 mL/min/1.73 m²或尿白蛋白排泄率超过300 mg/g尿肌酐时,将糖尿病患者转诊至肾脏病科。从概念上讲,当CKD患者功能性肾组织丢失超过70%时才被转诊至负责CKD防治的专科医生处,这显得有些奇怪。全球CKD健康负担不断增加,很大程度上是由DKD所致;与其他糖尿病并发症相比,常规治疗对DKD结局的影响欠佳;认识到CKD的成功治疗需要早期诊断和干预;肾脏损伤早期诊断方面的进展;以及最近出现的具有肾脏作用机制且无低血糖风险、同时具有心脏和肾脏保护作用的抗糖尿病药物,所有这些都表明糖尿病患者的护理模式需要转变,应作为协调和综合护理方法的一部分,更早地将他们转诊至肾脏病科。