Division of Infectious Diseases, Massachusetts General Hospital, Boston, Massachusetts, USA.
Medical Practice Evaluation Center, Massachusetts General Hospital, Boston, Massachusetts, USA.
Clin Infect Dis. 2021 Dec 16;73(12):2248-2256. doi: 10.1093/cid/ciab111.
Isolation of hospitalized persons under investigation (PUIs) for coronavirus disease 2019 (COVID-19) reduces nosocomial transmission risk. Efficient evaluation of PUIs is needed to preserve scarce healthcare resources. We describe the development, implementation, and outcomes of an inpatient diagnostic algorithm and clinical decision support system (CDSS) to evaluate PUIs.
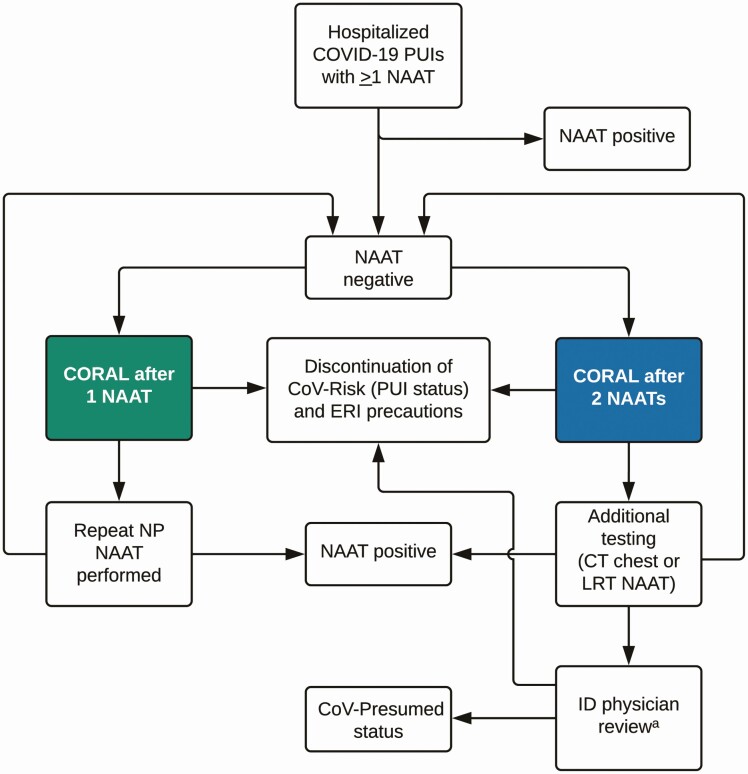
We conducted a pre-post study of CORAL (COvid Risk cALculator), a CDSS that guides frontline clinicians through a risk-stratified COVID-19 diagnostic workup, removes transmission-based precautions when workup is complete and negative, and triages complex cases to infectious diseases (ID) physician review. Before CORAL, ID physicians reviewed all PUI records to guide workup and precautions. After CORAL, frontline clinicians evaluated PUIs directly using CORAL. We compared pre- and post-CORAL frequency of repeated severe acute respiratory syndrome coronavirus 2 nucleic acid amplification tests (NAATs), time from NAAT result to PUI status discontinuation, total duration of PUI status, and ID physician work hours, using linear and logistic regression, adjusted for COVID-19 incidence.
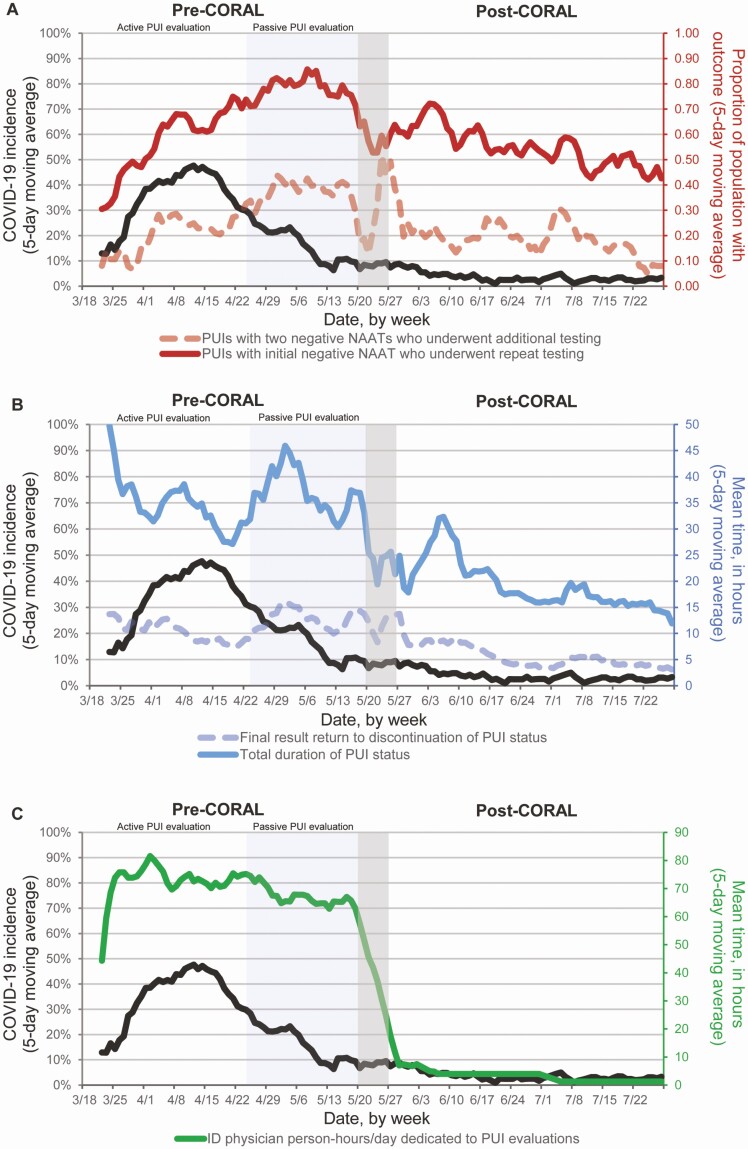
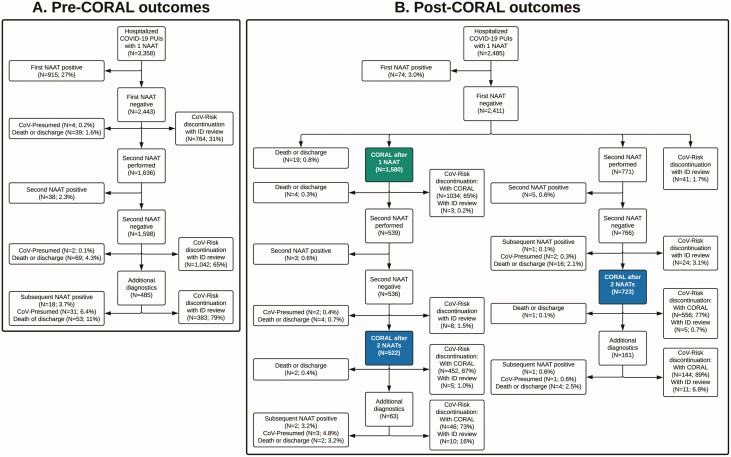
Fewer PUIs underwent repeated testing after an initial negative NAAT after CORAL than before CORAL (54% vs 67%, respectively; adjusted odd ratio, 0.53 [95% confidence interval, .44-.63]; P < .01). CORAL significantly reduced average time to PUI status discontinuation (adjusted difference [standard error], -7.4 [0.8] hours per patient), total duration of PUI status (-19.5 [1.9] hours per patient), and average ID physician work-hours (-57.4 [2.0] hours per day) (all P < .01). No patients had a positive NAAT result within 7 days after discontinuation of precautions via CORAL.
CORAL is an efficient and effective CDSS to guide frontline clinicians through the diagnostic evaluation of PUIs and safe discontinuation of precautions.
对 2019 年冠状病毒病(COVID-19)下住院的疑似患者(PUIs)进行隔离可降低医院内传播的风险。需要高效地评估 PUIs,以保护有限的医疗资源。我们描述了一种住院患者诊断算法和临床决策支持系统(CDSS)的开发、实施和结果,以评估 PUIs。
我们进行了 CORAL(COvid Risk cALculator)的前后研究,这是一种 CDSS,它通过风险分层 COVID-19 诊断工作流程指导一线临床医生,在工作流程完成且结果为阴性时消除基于传播的预防措施,并将复杂病例分诊给传染病(ID)医生进行审查。在 CORAL 之前,ID 医生审查所有 PUI 记录以指导工作流程和预防措施。在 CORAL 之后,一线临床医生直接使用 CORAL 评估 PUIs。我们使用线性和逻辑回归比较了 CORAL 前后重复严重急性呼吸综合征冠状病毒 2 核酸扩增试验(NAAT)的频率、从 NAAT 结果到 PUI 状态终止的时间、PUI 状态的总持续时间和 ID 医生的工作时间,调整了 COVID-19 的发病率。
与 CORAL 之前相比,CORAL 后首次阴性 NAAT 后接受重复检测的 PUI 减少(分别为 54%和 67%;调整后的比值比,0.53[95%置信区间,0.44-0.63];P<0.01)。CORAL 显著缩短了 PUI 状态终止的平均时间(调整后的差异[标准误差],-7.4[0.8]小时/患者)、PUI 状态的总持续时间(-19.5[1.9]小时/患者)和 ID 医生的平均工作时间(-57.4[2.0]小时/天)(均 P<0.01)。没有患者在通过 CORAL 停止预防措施后 7 天内出现阳性 NAAT 结果。
CORAL 是一种高效、有效的 CDSS,可指导一线临床医生对 PUIs 进行诊断评估,并安全地停止预防措施。