van den Munckhof Pepijn, Bot Maarten, Schuurman P Richard
Department of Neurosurgery, Amsterdam University Medical Centers, Academic Medical Center (AMC), Amsterdam, The Netherlands.
Neurol Ther. 2021 Jun;10(1):61-73. doi: 10.1007/s40120-021-00233-8. Epub 2021 Feb 9.
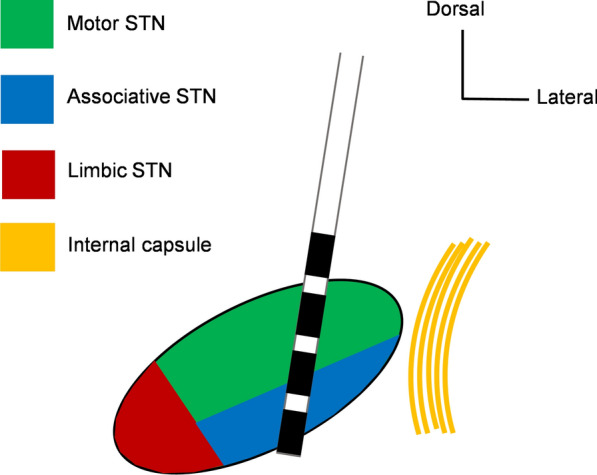
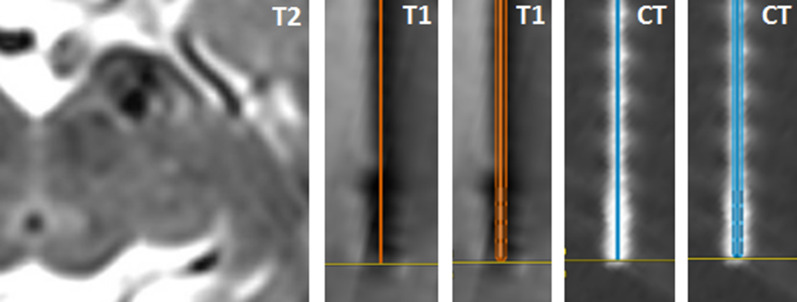
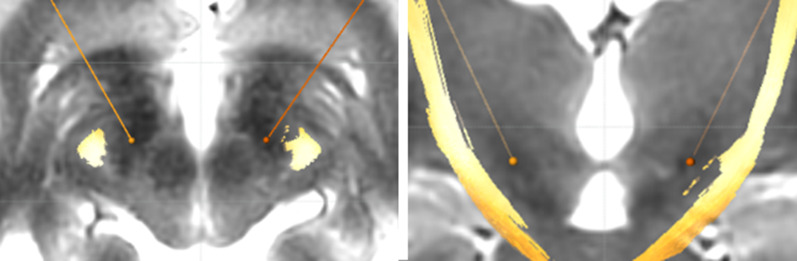
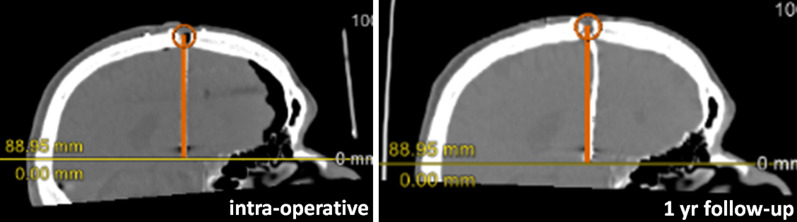
Precise stereotactic targeting of the dorsolateral motor part of the subthalamic nucleus (STN) is paramount for maximizing clinical effectiveness and preventing side effects of deep brain stimulation (DBS) in patients with advanced Parkinson's disease. With recent developments in magnetic resonance imaging (MRI) techniques, direct targeting of the dorsolateral part of the STN is now feasible, together with visualization of the motor fibers in the nearby internal capsule. However, clinically relevant discrepancies were reported when comparing STN borders on MRI to electrophysiological STN borders during microelectrode recordings (MER). Also, one should take into account the possibility of a 3D inaccuracy of up to 2 mm of the applied stereotactic technique. Pneumocephalus and image fusion errors may further increase implantation inaccuracy. Even when implantation has been successful, suboptimal lead anchoring on the skull may cause lead migration during follow-up. Meticulous pre- and intraoperative imaging is therefore indispensable, and so is postoperative imaging when the effects of DBS deteriorate during follow-up. Thus far, most DBS centers employ MRI targeting, multichannel MER, and awake test stimulation in STN surgery, but randomized trials comparing surgery under local versus general anesthesia and additional studies comparing MER-STN borders to high-field MRI-STN may change this clinical practice. Further developments in imaging protocols and improvements in image fusion processes are needed to optimize placement of DBS leads in the dorsolateral motor part of the STN in Parkinson's disease.
对于晚期帕金森病患者,精确立体定向靶向丘脑底核(STN)的背外侧运动部分对于最大化临床疗效和预防深部脑刺激(DBS)的副作用至关重要。随着磁共振成像(MRI)技术的最新发展,现在可以直接靶向STN的背外侧部分,并可视化附近内囊中的运动纤维。然而,在微电极记录(MER)期间,将MRI上的STN边界与电生理STN边界进行比较时,报告了临床相关的差异。此外,应考虑到所应用的立体定向技术可能存在高达2毫米的三维误差。气颅和图像融合误差可能会进一步增加植入的不准确性。即使植入成功,颅骨上铅锚定不佳也可能导致随访期间铅移位。因此,细致的术前和术中成像不可或缺,当DBS的效果在随访期间恶化时,术后成像也是如此。到目前为止,大多数DBS中心在STN手术中采用MRI靶向、多通道MER和清醒测试刺激,但比较局部麻醉与全身麻醉下手术的随机试验以及比较MER-STN边界与高场MRI-STN的其他研究可能会改变这种临床实践。需要成像方案的进一步发展和图像融合过程的改进,以优化帕金森病患者DBS电极在STN背外侧运动部分的放置。