Sachdev Rani, Field Mike, Baynam Gareth S, Beilby John, Berarducci Maria, Berman Yemima, Boughtwood Tiffany, Cusack Marie B, Fitzgerald Vanessa, Fletcher Jeffery, Freckmann Mary-Louise, Grainger Natalie, Kirk Edwin, Lundie Ben, Lunke Sebastian, McGregor Lesley, Mowat David, Parasivam Gayathri, Tyrell Vanessa, Wallis Mathew, White Susan M, S L Ma Alan
Centre for Clinical Genetics, Sydney Children's Hospital-Randwick, Sydney Children's Hospitals Network, Sydney, New South Wales, Australia.
School of Women's and Children's Health, University of New South Wales, Sydney, New South Wales, Australia.
J Paediatr Child Health. 2021 Apr;57(4):477-483. doi: 10.1111/jpc.15382. Epub 2021 Feb 10.
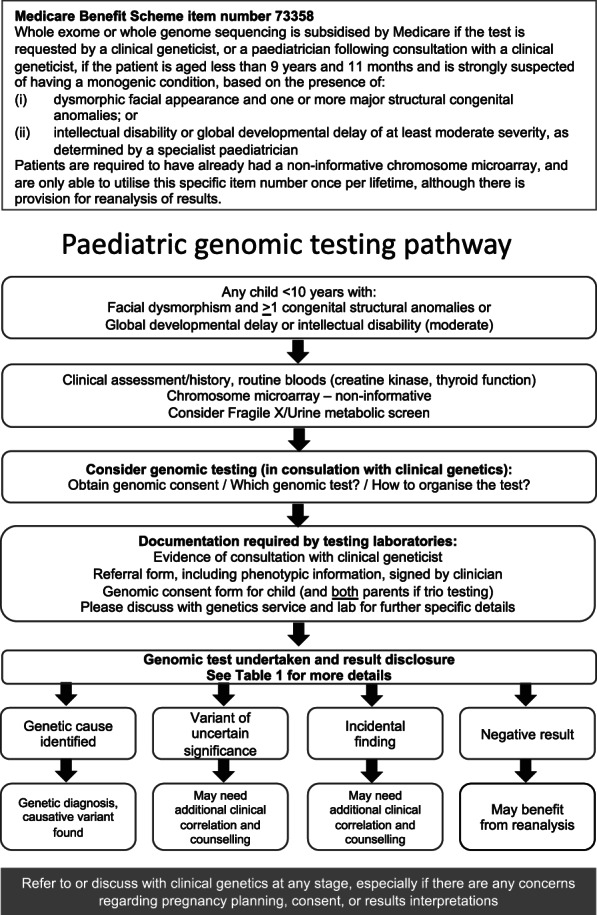
Genomic testing for a genetic diagnosis is becoming standard of care for many children, especially those with a syndromal intellectual disability. While previously this type of specialised testing was performed mainly by clinical genetics teams, it is increasingly being 'mainstreamed' into standard paediatric care. With the introduction of a new Medicare rebate for genomic testing in May 2020, this type of testing is now available for paediatricians to order, in consultation with clinical genetics. Children must be aged less than 10 years with facial dysmorphism and multiple congenital abnormalities or have global developmental delay or moderate to severe intellectual disability. This rebate should increase the likelihood of a genetic diagnosis, with accompanying benefits for patient management, reproductive planning and diagnostic certainty. Similar to the introduction of chromosomal microarray into mainstream paediatrics, this genomic testing will increase the number of genetic diagnoses, however, will also yield more variants of uncertain significance, incidental findings, and negative results. This paper aims to guide paediatricians through the process of genomic testing, and represents the combined expertise of educators, clinical geneticists, paediatricians and genomic pathologists around Australia. Its purpose is to help paediatricians navigate choosing the right genomic test, consenting patients and understanding the possible outcomes of testing.
基因检测用于遗传诊断正成为许多儿童的标准治疗手段,尤其是那些患有综合征型智力障碍的儿童。此前,这类专门检测主要由临床遗传学团队进行,如今它正越来越多地被“纳入”标准儿科护理。随着2020年5月针对基因检测推出新的医疗保险回扣,现在儿科医生在与临床遗传学专家协商后即可开具此类检测。儿童必须年龄小于10岁,有面部畸形和多种先天性异常,或有全面发育迟缓或中度至重度智力障碍。这种回扣应会增加做出遗传诊断的可能性,对患者管理、生育规划和诊断确定性都有相应益处。与将染色体微阵列引入主流儿科类似,这种基因检测将增加遗传诊断的数量,然而,也会产生更多意义不明确的变异、偶然发现和阴性结果。本文旨在指导儿科医生完成基因检测过程,它代表了澳大利亚各地教育工作者、临床遗传学家、儿科医生和基因病理学家的综合专业知识。其目的是帮助儿科医生在选择正确的基因检测、征得患者同意以及理解检测可能结果方面做出正确决策。