Specka Michael, Groll Maria, Scherbaum Norbert, Wiltfang Jens, Benninghoff Jens
LVR-Klinikum Essen, Klinik für Psychiatrie und Psychotherapie, Universität Duisburg-Essen, Duisburg-Essen, Deutschland.
Klinik für Psychiatrie und Psychotherapie, Universitätsmedizin Göttingen, Göttingen, Deutschland.
Z Gerontol Geriatr. 2022 May;55(3):231-238. doi: 10.1007/s00391-021-01850-6. Epub 2021 Feb 11.
Multimorbidity in old age is one reason for intensified pharmacotherapy. At the same time, an increase in medications could augment multimorbidity, especially when drug interactions leading to undesired drug effects occur.
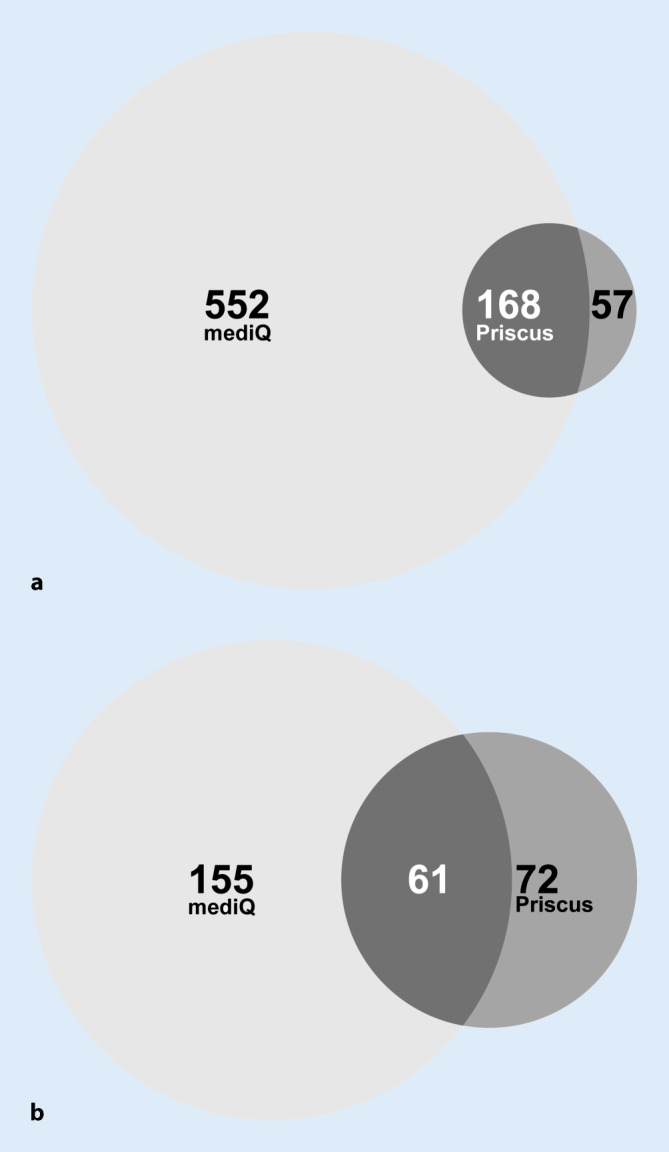
In this cross-sectional study 918 mentally ill seniors living in nursing homes (mean age 79.3 (±11.6) years; 31.8% male) were included. Two different approaches to assess risks due to pharmacotherapy were applied: first mediQ, an online-based clinical decision support software (CDSS) and the PRISCUS list, which indicates potentially inappropriate medication. PRISCUS is the German equivalent to the American Geriatrics Society Beers criteria.
Of the patients in the study 76.3% were at clinical risk, 2.2% at potentially high risk for drug interactions regarding the entire medication as tested by mediQ, and about 25% of the studied population received potentially inappropriate medication according to the PRISCUS list.
This difference clearly underlines the cumbersome complexity of identifying patients at risk by using these exemplary devices. The focus of avoiding undesired drug side effects should be taking medication only after thorough verification of clinical indications and under close monitoring. The CDSS or negative lists may support this process.
老年多病共存是强化药物治疗的一个原因。与此同时,药物数量的增加可能会加重多病共存的情况,尤其是当发生导致不良药物效应的药物相互作用时。
在这项横断面研究中,纳入了918名居住在养老院的患有精神疾病的老年人(平均年龄79.3(±11.6)岁;男性占31.8%)。应用了两种不同的方法来评估药物治疗带来的风险:第一种是mediQ,一个基于网络的临床决策支持软件(CDSS),以及PRISCUS清单,该清单指出了潜在不适当的药物。PRISCUS相当于美国老年医学会的Beers标准的德国版本。
在研究中的患者里,76.3%处于临床风险中,通过mediQ测试,就整个用药情况而言,2.2%处于药物相互作用的潜在高风险中,并且根据PRISCUS清单,约25%的研究人群接受了潜在不适当的药物治疗。
这种差异清楚地凸显了使用这些示例工具识别有风险患者的繁琐复杂性。避免不良药物副作用的重点应该是在彻底核实临床指征后并在密切监测下用药。临床决策支持软件或负面清单可能有助于这一过程。