Tedeschi Sara K, Sobiesczyzk Piotr S, Ford Julia A, DiIorio Michael A, Docken William P
Harvard Medical School and Brigham and Women's Hospital, Boston, Massachusetts.
University of Michigan, Ann Arbor.
ACR Open Rheumatol. 2021 Mar;3(3):147-153. doi: 10.1002/acr2.11227. Epub 2021 Feb 11.
Vascular ultrasound (VUS) is a first-line test for giant cell arteritis (GCA) in Europe but has been of limited use in the United States. We report clinical experience with a multidisciplinary model of VUS for the evaluation of GCA at a large US medical center.
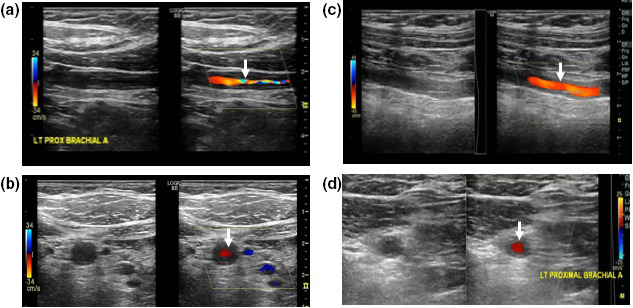
Patients who underwent VUS for evaluation of GCA between 2013 and 2017 were reviewed. Trained vascular technologists followed a standardized protocol to visualize bilateral temporal, carotid, subclavian, and axillary arteries. Vascular medicine physicians interpreted VUS as no arteritis, hyperechoic wall thickening, or acute arteritis. Characteristics of patients with versus without acute arteritis (no arteritis or hyperechoic wall thickening) were compared. Among patients with suspected new-onset GCA, the treating physician's pretest and posttest suspicion for GCA were compared.
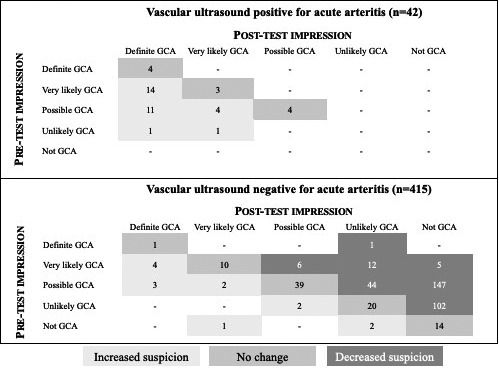
Of 530 patients, 10.6% had prior-onset GCA, 31.7% had polymyalgia rheumatica, and 57.6% were taking glucocorticoids. Most patients had no arteritis on VUS (84.3%); 10.6% had acute arteritis, and 5.1% had hyperechoic wall thickening. Typical GCA symptoms, such as jaw claudication and scalp tenderness, were significantly more frequent in patients with acute arteritis. For all 42 patients with suspected new-onset GCA and acute arteritis, posttest suspicion was unchanged or increased. Of 415 patients with suspected new-onset GCA and VUS without acute arteritis, suspicion decreased (76.4%) or was unchanged (20.2%).
We describe a multidisciplinary model for incorporating VUS into GCA care. When pretest suspicion was low and VUS did not reveal acute arteritis, posttest suspicion typically decreased, whereas when pretest suspicion was high and VUS revealed acute arteritis, posttest suspicion was reinforced.
血管超声(VUS)在欧洲是巨细胞动脉炎(GCA)的一线检测方法,但在美国其应用有限。我们报告了美国一家大型医疗中心采用多学科VUS模型评估GCA的临床经验。
回顾了2013年至2017年间接受VUS评估GCA的患者。训练有素的血管技术人员遵循标准化方案对双侧颞动脉、颈动脉、锁骨下动脉和腋动脉进行可视化检查。血管内科医生将VUS解读为无动脉炎、高回声壁增厚或急性动脉炎。比较了有急性动脉炎(无动脉炎或高回声壁增厚)和无急性动脉炎患者的特征。在疑似新发GCA的患者中,比较了治疗医生检查前和检查后对GCA的怀疑程度。
530例患者中,10.6%有既往发作的GCA,31.7%有风湿性多肌痛,57.6%正在服用糖皮质激素。大多数患者VUS显示无动脉炎(84.3%);10.6%有急性动脉炎,5.1%有高回声壁增厚。急性动脉炎患者出现典型GCA症状(如颌部间歇性运动障碍和头皮压痛)的频率明显更高。对于所有42例疑似新发GCA且有急性动脉炎的患者,检查后的怀疑程度未改变或增加。在415例疑似新发GCA且VUS显示无急性动脉炎的患者中,怀疑程度降低(76.4%)或未改变(20.2%)。
我们描述了一种将VUS纳入GCA护理的多学科模型。当检查前怀疑程度较低且VUS未显示急性动脉炎时,检查后怀疑程度通常会降低,而当检查前怀疑程度较高且VUS显示急性动脉炎时,检查后怀疑程度会增强。