School of Medicine Pontifical Catholic University of Paraná, Curitiba, Paraná PR, Brazil.
Marcelino Champagnat Hospital, Curitiba, Paraná PR, Brazil.
PLoS One. 2021 Feb 12;16(2):e0246837. doi: 10.1371/journal.pone.0246837. eCollection 2021.
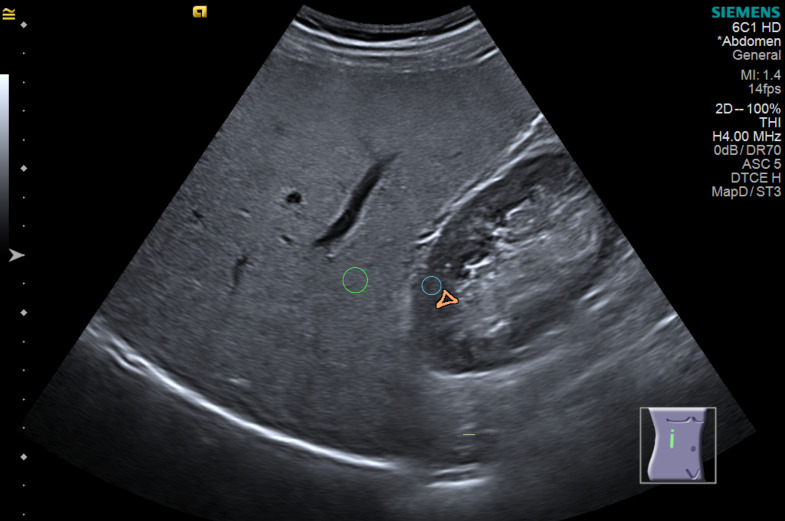
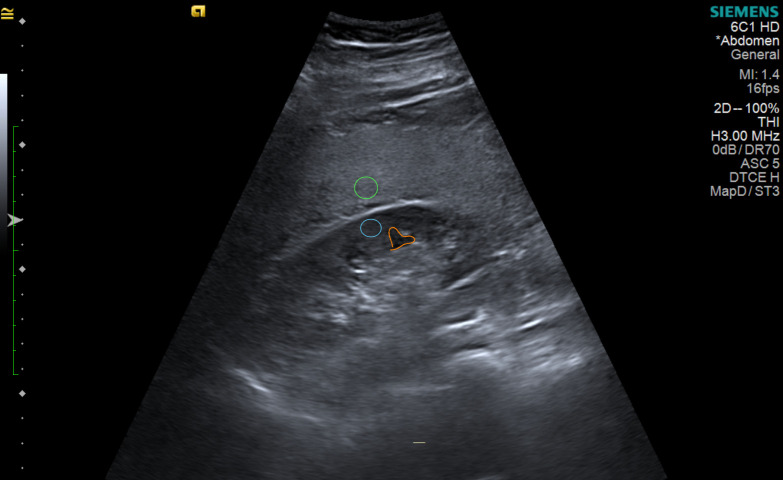
Ultrasonography is widely used as the first tool to evaluate fatty liver disease, and the hepatorenal index is a semi-quantitative method that improves its performance. Fibrosis can co-exist with steatosis or even replace it during disease progression. This study aimed to evaluate the influence of fibrosis on the measurement of steatosis using the hepatorenal index.
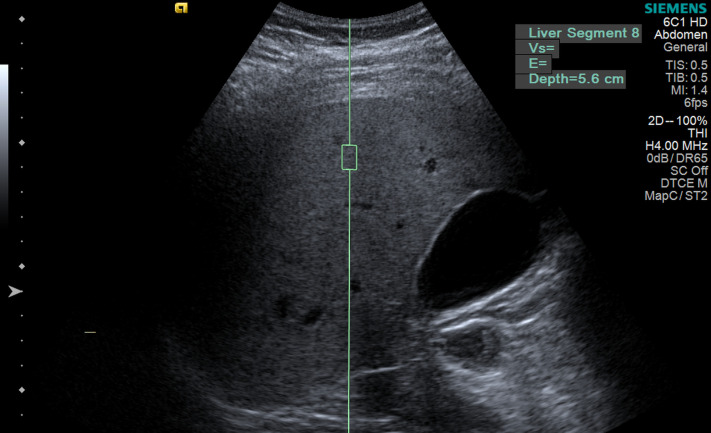
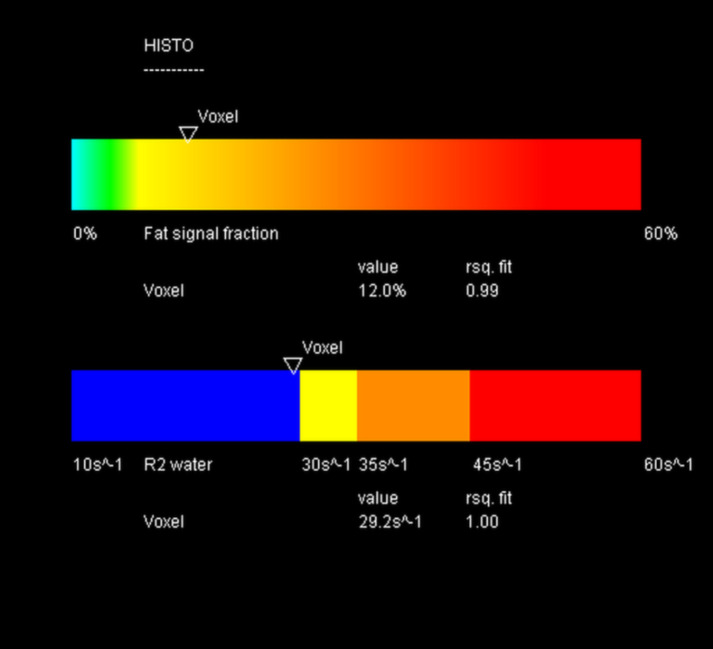
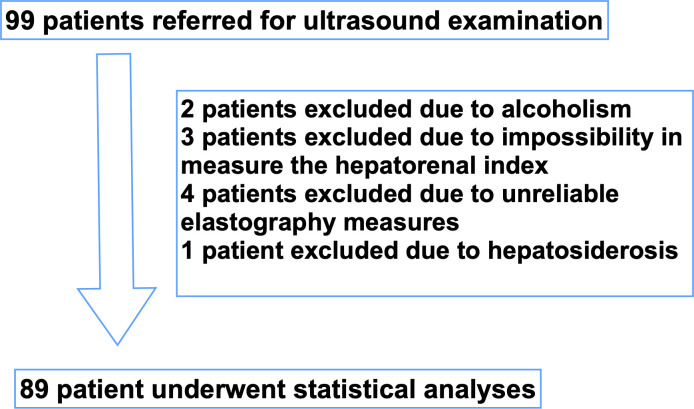
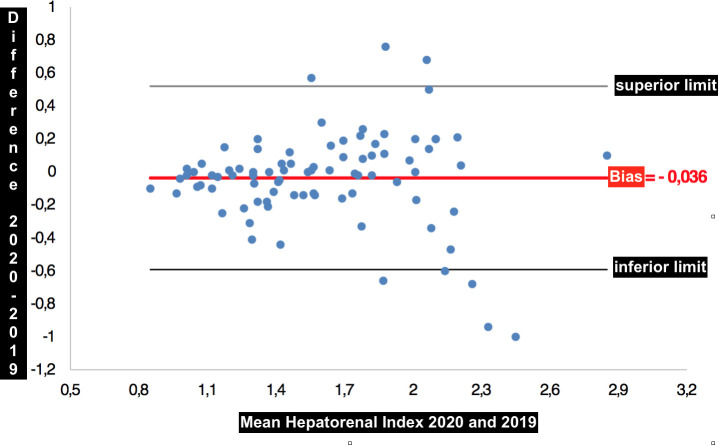
This cross-sectional study included 89 patients with nonalcoholic fatty liver disease and in whom liver fibrosis was determined by ultrasound elastography. The Pearson's correlation coefficient was used to compare between the results of the sonographic hepatorenal index and the quantification of steatosis using magnetic resonance spectroscopy as well the accuracy of detecting moderate to severe steatosis using sonography in two groups of patients: (A) without advanced fibrosis and (B) with advanced fibrosis. Advanced fibrosis was defined as a shear wave speed ≥ 1.78 m/s on ultrasound elastography. We calculated the area under the curve (AUC-ROC) to detect the ability of the hepatorenal index to differentiate light from moderate to severe steatosis in both groups. Moderate to severe steatosis was defined as a fat fraction > 15% on the magnetic resonance spectroscopy. The intra-observer variability was assessed using the Bland-Altman plot.
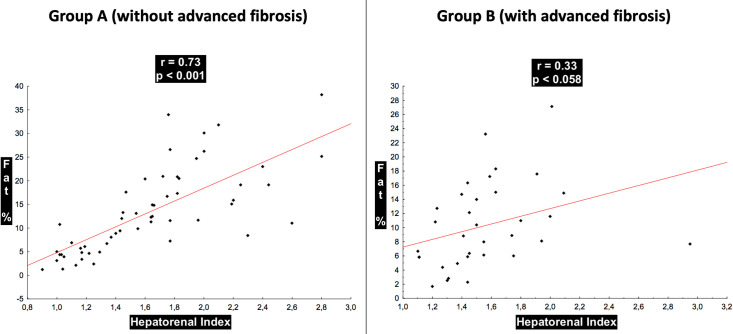
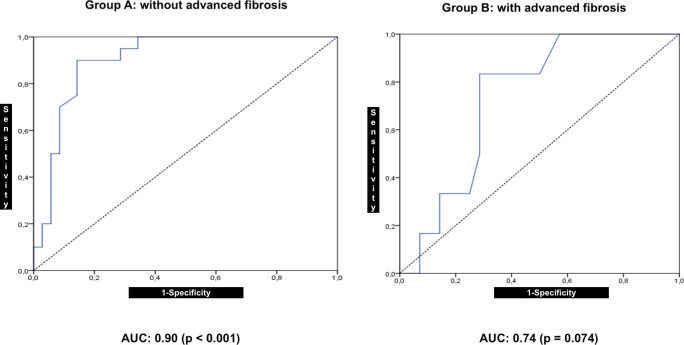
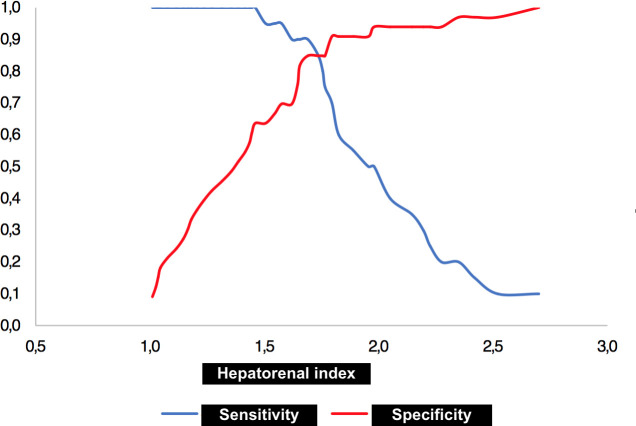
Among patients, the mean age was 54.6 years and 59.6% were women, 50.6% had a body mass index ≥ 30 kg/m2, 29.2% had moderate to severe steatosis, and 27.2% had advanced fibrosis. There was a correlation between steatosis grading by ultrasonography and magnetic resonance in group A (0.73; P < 0.001), but not in Group B (0.33; P = 0.058). The AUC-ROC for detecting a steatosis fraction ≥ 15% was 0.90 and 0.74 in group A and group B, respectively. The intra-observer variability for the hepatorenal index measurements was not significant (-0.036; P = 0.242).
The hepatorenal index is not appropriate for estimating steatosis in livers with advanced fibrosis.
超声检查广泛用于评估脂肪肝疾病,而肝肾指数是一种半定量方法,可提高其性能。纤维化可能与脂肪变性并存,甚至在疾病进展过程中取代脂肪变性。本研究旨在评估纤维化对肝肾指数测量脂肪变性的影响。
这是一项横断面研究,共纳入 89 例非酒精性脂肪性肝病患者,采用超声弹性成像检测肝纤维化。采用 Pearson 相关系数比较两组患者的超声肝肾指数与磁共振波谱定量脂肪变性的结果:(A)无晚期纤维化患者和(B)有晚期纤维化患者。晚期纤维化定义为超声弹性成像剪切波速度≥1.78m/s。我们计算了曲线下面积(AUC-ROC)以检测肝肾指数在两组患者中区分轻度与中重度脂肪变性的能力。中重度脂肪变性定义为磁共振波谱脂肪分数>15%。采用 Bland-Altman 图评估观察者内变异性。
患者的平均年龄为 54.6 岁,59.6%为女性,50.6%的体重指数≥30kg/m2,29.2%有中重度脂肪变性,27.2%有晚期纤维化。在组 A 中,超声检查的脂肪变性分级与磁共振检查有相关性(0.73;P<0.001),但在组 B 中无相关性(0.33;P=0.058)。在组 A 和组 B 中,检测脂肪分数≥15%的 AUC-ROC 分别为 0.90 和 0.74。肝肾指数测量的观察者内变异性不显著(-0.036;P=0.242)。
肝肾指数不适用于评估晚期纤维化肝脏的脂肪变性。