Department of Interventional Therapy, Beijing Shijitan Hospital, Capital Medical University, Beijing 100038, China.
World J Gastroenterol. 2021 Feb 7;27(5):416-427. doi: 10.3748/wjg.v27.i5.416.
Hepatic encephalopathy (HE) remains an enormous challenge in patients who undergo transjugular intrahepatic portosystemic shunt (TIPS) implantation. The preoperative indocyanine green retention rate at 15 min (ICG-R15), as one of the liver function assessment tools, has been developed as a prognostic indicator in patients undergoing surgery, but there are limited data on its role in TIPS.
To determine whether the ICG-R15 can be used for prediction of post-TIPS HE in decompensated cirrhosis patients with portal hypertension (PHT) and compare the clinical value of ICG-R15, Child-Pugh score (CPS), and model for end-stage liver disease (MELD) score in predicting post-TIPS HE with PHT.
This retrospective study included 195 patients with PHT who underwent elective TIPS at Beijing Shijitan Hospital from January 2018 to June 2019. All patients underwent the ICG-R15 test, CPS evaluation, and MELD scoring 1 wk before TIPS. According to whether they developed HE or not, the patients were divided into two groups: HE group and non-HE group. The prediction of one-year post-TIPS HE by ICG-R15, CPS and MELD score was evaluated by the areas under the receiver operating characteristic curves (AUCs).
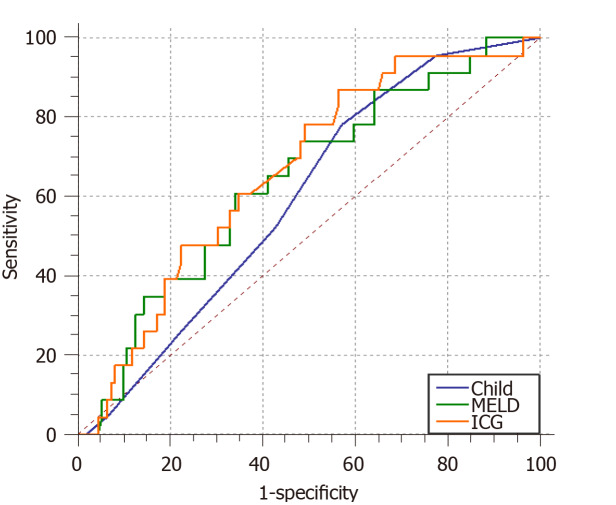
A total of 195 patients with portal hypertension were included and 23% (45/195) of the patients developed post-TIPS HE. The ICG-R15 was identified as an independent predictor of post-TIPS HE. The AUCs for the ICG-R15, CPS, and MELD score for predicting post-TIPS HE were 0.664 (95% confidence interval [CI]: 0.557-0.743, = 0.0046), 0.596 (95%CI: 0.508-0.679, = 0.087), and 0.641 (95%CI: 0.554-0.721, = 0.021), respectively. The non-parametric approach (Delong-Delong & Clarke-Pearson) showed that there was statistical significance in pairwise comparison between AUCs of ICG-R15 and MELD score ( = 0.0229).
The ICG-R15 has appreciated clinical value for predicting the occurrence of post-TIPS HE and is a choice for evaluating the prognosis of patients undergoing TIPS.
经颈静脉肝内门体分流术(TIPS)植入后,肝性脑病(HE)仍然是患者面临的巨大挑战。作为肝功能评估工具之一的 15 分钟吲哚菁绿滞留率(ICG-R15)已被确定为手术患者的预后指标,但关于其在 TIPS 中的作用的数据有限。
确定 ICG-R15 是否可用于预测代偿性肝硬化伴门静脉高压(PHT)患者 TIPS 后 HE,并比较 ICG-R15、Child-Pugh 评分(CPS)和终末期肝病模型(MELD)评分在预测 PHT 患者 TIPS 后 HE 中的临床价值。
本回顾性研究纳入了 2018 年 1 月至 2019 年 6 月在北京世纪坛医院接受择期 TIPS 的 195 例 PHT 患者。所有患者在 TIPS 前 1 周内均进行了 ICG-R15 试验、CPS 评估和 MELD 评分。根据是否发生 HE,患者分为 HE 组和非 HE 组。通过受试者工作特征曲线下面积(AUCs)评估 ICG-R15、CPS 和 MELD 评分对 TIPS 后 1 年 HE 的预测能力。
共纳入 195 例 PHT 患者,23%(45/195)患者发生 TIPS 后 HE。ICG-R15 是 TIPS 后 HE 的独立预测因子。ICG-R15、CPS 和 MELD 评分预测 TIPS 后 HE 的 AUC 分别为 0.664(95%置信区间 [CI]:0.557-0.743, = 0.0046)、0.596(95%CI:0.508-0.679, = 0.087)和 0.641(95%CI:0.554-0.721, = 0.021)。非参数方法(Delong-Delong 和 Clarke-Pearson)显示,ICG-R15 和 MELD 评分之间的 AUC 比较存在统计学意义( = 0.0229)。
ICG-R15 对预测 TIPS 后 HE 的发生具有较高的临床价值,是评估 TIPS 患者预后的选择之一。