Versace Viviana, Sebastianelli Luca, Ferrazzoli Davide, Saltuari Leopold, Kofler Markus, Löscher Wolfgang, Uncini Antonino
Department of Neurorehabilitation, Hospital of Vipiteno (SABES-ASDAA), Vipiteno, Italy.
Department of Neurology, Hochzirl Hospital, Zirl, Austria.
Front Neurol. 2021 Jan 29;12:625144. doi: 10.3389/fneur.2021.625144. eCollection 2021.
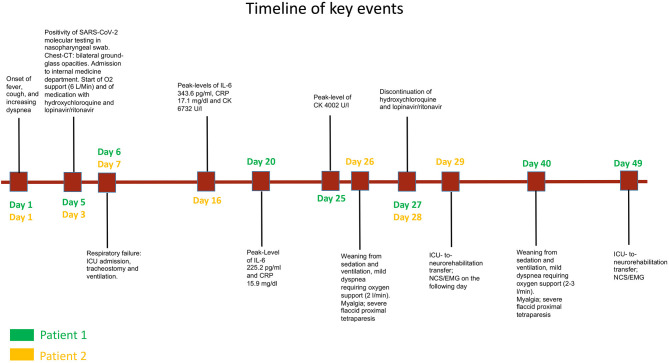
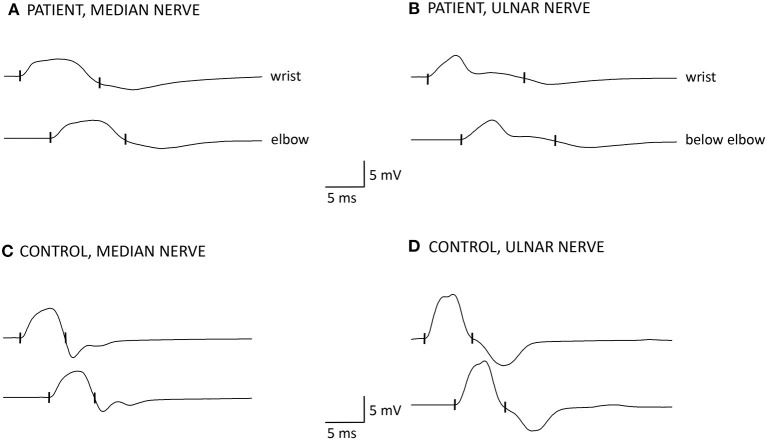
COVID-19-associated muscular complications may comprise myalgia, weakness, wasting, and rhabdomyolysis. Skeletal muscle damage in COVID-19 may be due to direct infection by the virus SARS-CoV-2 through interaction with the ACE2 receptor, systemic hyper-inflammatory state with cytokine release and homeostatic perturbation, an autoimmune process, or myotoxic drugs. Disclosing the cause of weakness in an individual patient is therefore difficult. We report two patients, who survived typical COVID-19 pneumonia requiring intensive care treatment and who developed early on myalgia and severe proximal weakness in all four limbs. Laboratory exams revealed elevated serum creatine kinase and markedly increased C-reactive protein and interleukin 6, concurring with a systemic inflammatory response. On admission in neurorehabilitation (4 and 7 weeks after COVID-19 onset, respectively), the patients presented with proximal flaccid tetraparesis and limb-girdle muscle atrophy. Motor nerve conduction studies showed decreased amplitude and prolonged duration of compound muscle action potentials (CMAPs) with normal distal motor latencies and normal conduction velocities in median and ulnar nerves. Needle electromyography in proximal muscles revealed spontaneous activity in one and myopathic changes in both patients. Clinical, laboratory, and electrodiagnostic findings in these patients were unequivocally consistent with myopathy. Interestingly, increased distal CMAP duration has been described in patients with critical illness myopathy (CIM) and reflects slow muscle fiber conduction velocity due to membrane hypo-excitability, possibly induced by inflammatory cytokines. By analogy with CIM, the pathogenesis of COVID-19-related myopathy might also depend on hyperinflammation and metabolic pathways that may affect muscles in a pathophysiological continuum from hypo-excitability to necrosis.
新型冠状病毒肺炎(COVID-19)相关的肌肉并发症可能包括肌痛、肌无力、肌肉萎缩和横纹肌溶解。COVID-19患者的骨骼肌损伤可能是由于严重急性呼吸综合征冠状病毒2(SARS-CoV-2)通过与血管紧张素转换酶2(ACE2)受体相互作用直接感染、细胞因子释放导致的全身高炎症状态和内环境紊乱、自身免疫过程或具有肌毒性的药物。因此,要明确个体患者肌无力的病因很困难。我们报告了两名患者,他们均从需要重症监护治疗的典型COVID-19肺炎中康复,且在病程早期就出现了肌痛和四肢严重近端肌无力。实验室检查显示血清肌酸激酶升高,C反应蛋白和白细胞介素6显著增加,这与全身炎症反应一致。在进入神经康复治疗时(分别在COVID-19发病后4周和7周),这两名患者均表现为近端弛缓性四肢瘫和肢带肌萎缩。运动神经传导研究显示复合肌肉动作电位(CMAP)波幅降低、时限延长,而正中神经和尺神经的远端运动潜伏期正常、传导速度正常。近端肌肉的针极肌电图显示,其中一名患者有自发电活动,两名患者均有肌病性改变。这些患者的临床、实验室和电诊断结果明确显示与肌病相符。有趣的是,危重症性肌病(CIM)患者也有远端CMAP时限增加的情况,这反映了由于膜兴奋性降低导致的肌纤维传导速度减慢,可能是由炎性细胞因子引起的。与CIM类似,COVID-19相关肌病的发病机制也可能取决于高炎症反应和代谢途径,这些因素可能在从兴奋性降低到坏死的病理生理连续过程中影响肌肉。