Department of Neurosurgery, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
CTU Bern, University of Bern, Bern, Switzerland.
J Cachexia Sarcopenia Muscle. 2022 Jun;13(3):1883-1895. doi: 10.1002/jcsm.12989. Epub 2022 Apr 5.
The COVID-19 pandemic has greatly increased the incidence and clinical importance of critical illness myopathy (CIM), because it is one of the most common complications of modern intensive care medicine. Current diagnostic criteria only allow diagnosis of CIM at an advanced stage, so that patients are at risk of being overlooked, especially in early stages. To determine the frequency of CIM and to assess a recently proposed tool for early diagnosis, we have followed a cohort of COVID-19 patients with acute respiratory distress syndrome and compared the time course of muscle excitability measurements with the definite diagnosis of CIM.
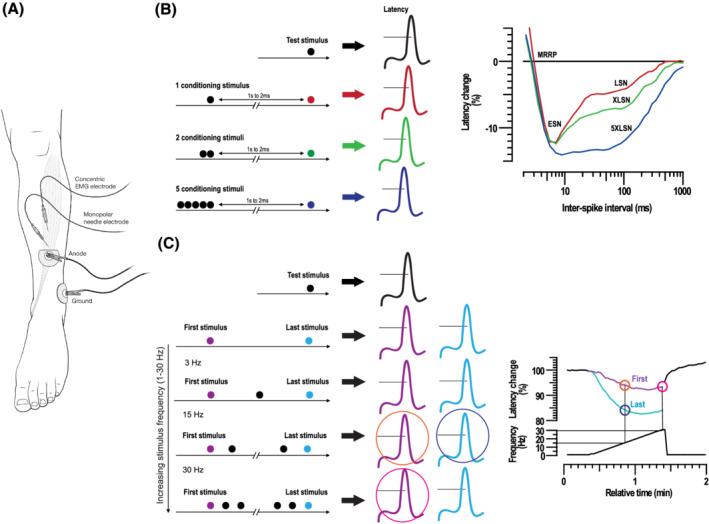
Adult COVID-19 patients admitted to the Intensive Care Unit of the University Hospital Bern, Switzerland requiring mechanical ventilation were recruited and examined on Days 1, 2, 5, and 10 post-intubation. Clinical examination, muscle excitability measurements, medication record, and laboratory analyses were performed on all study visits, and additionally nerve conduction studies, electromyography and muscle biopsy on Day 10. Muscle excitability data were compared with a cohort of 31 age-matched healthy subjects. Diagnosis of definite CIM was made according to the current guidelines and was based on patient history, results of clinical and electrophysiological examinations as well as muscle biopsy.
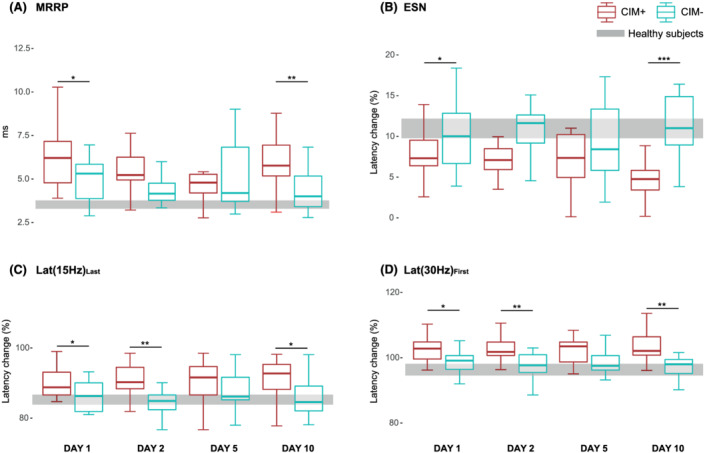
Complete data were available in 31 out of 44 recruited patients (mean [SD] age, 62.4 [9.8] years). Of these, 17 (55%) developed CIM. Muscle excitability measurements on Day 10 discriminated between patients who developed CIM and those who did not, with a diagnostic precision of 90% (AUC 0.908; 95% CI 0.799-1.000; sensitivity 1.000; specificity 0.714). On Days 1 and 2, muscle excitability parameters also discriminated between the two groups with 73% (AUC 0.734; 95% CI 0.550-0.919; sensitivity 0.562; specificity 0.857) and 82% (AUC 0.820; CI 0.652-0.903; sensitivity 0.750; specificity 0.923) diagnostic precision, respectively. All critically ill COVID-19 patients showed signs of muscle membrane depolarization compared with healthy subjects, but in patients who developed CIM muscle membrane depolarization on Days 1, 2 and 10 was more pronounced than in patients who did not develop CIM.
This study reports a 55% prevalence of definite CIM in critically ill COVID-19 patients. Furthermore, the results confirm that muscle excitability measurements may serve as an alternative method for CIM diagnosis and support its use as a tool for early diagnosis and monitoring the development of CIM.
COVID-19 大流行极大地增加了危重病肌病(CIM)的发病率和临床重要性,因为它是现代重症监护医学中最常见的并发症之一。目前的诊断标准仅允许在晚期诊断 CIM,因此患者有被忽视的风险,尤其是在早期。为了确定 CIM 的频率,并评估最近提出的早期诊断工具,我们对一组患有急性呼吸窘迫综合征的 COVID-19 患者进行了随访,并将肌肉兴奋性测量的时间过程与 CIM 的明确诊断进行了比较。
瑞士伯尔尼大学医院重症监护病房收治的需要机械通气的成年 COVID-19 患者被招募并在插管后第 1、2、5 和 10 天进行检查。所有研究访视时均进行临床检查、肌肉兴奋性测量、用药记录和实验室分析,另外在第 10 天进行神经传导研究、肌电图和肌肉活检。肌肉兴奋性数据与 31 名年龄匹配的健康对照进行比较。根据当前指南诊断明确的 CIM,并基于患者病史、临床和电生理检查结果以及肌肉活检结果。
44 名入组患者中,31 名(平均[标准差]年龄,62.4[9.8]岁)完成了完整的数据采集。其中,17 名(55%)患者发生了 CIM。第 10 天的肌肉兴奋性测量可区分发生 CIM 和未发生 CIM 的患者,诊断精度为 90%(AUC 0.908;95%CI 0.799-1.000;敏感度 1.000;特异性 0.714)。第 1 天和第 2 天,肌肉兴奋性参数也能区分两组,诊断精度分别为 73%(AUC 0.734;95%CI 0.550-0.919;敏感度 0.562;特异性 0.857)和 82%(AUC 0.820;CI 0.652-0.903;敏感度 0.750;特异性 0.923)。与健康对照组相比,所有重症 COVID-19 患者均表现出肌肉细胞膜去极化的迹象,但在发生 CIM 的患者中,第 1、2 和 10 天的肌肉细胞膜去极化程度比未发生 CIM 的患者更严重。
本研究报告了危重病 COVID-19 患者中明确 CIM 的发生率为 55%。此外,结果证实肌肉兴奋性测量可作为 CIM 诊断的替代方法,并支持将其用作早期诊断和监测 CIM 发展的工具。