Department of Neurology Yale University School of Medicine New Haven CT.
Department of Epidemiology Johns Hopkins Bloomberg School of Public Health Baltimore MD.
J Am Heart Assoc. 2021 Feb;10(5):e014270. doi: 10.1161/JAHA.120.014270. Epub 2021 Feb 15.
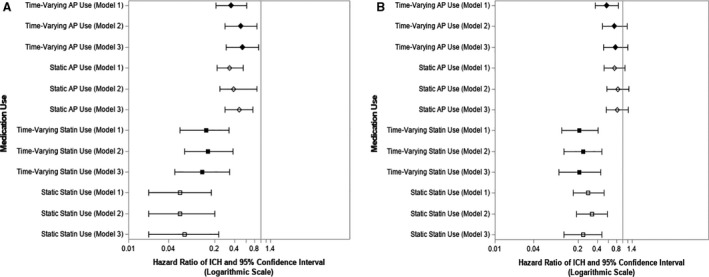
Background Antiplatelets, anticoagulants, and statins are commonly prescribed for various indications. The associations between these medications and the risk of intracerebral hemorrhage (ICH) and cerebral microbleeds (CMBs) are unclear. Methods and Results We performed a retrospective study of the ARIC (Atherosclerosis Risk in Communities) study cohort, recruited from 4 US communities in 1987 to 1989 with follow-up. In 2011 to 2013, a subset (N=1942) underwent brain magnetic resonance imaging with CMB evaluation. Time-varying and any antiplatelet, anticoagulant, or statin use was evaluated at subsequent study visits in participants not on each medication at baseline. To determine the hazard of ICH and odds of CMB by medication use, logistic and Cox proportional hazard models were built, respectively, adjusting for the propensity to take the medication, concomitant use of other medications, and cognitive, genetic, and radiographic data. Of 15 719 individuals during up to 20 years of follow-up, 130 participants experienced an ICH. The adjusted hazard of ICH was significantly lower among participants taking an antiplatelet at the most recent study visit before ICH versus nonusers (hazard ratio [HR], 0.53; 95% CI, 0.30-0.92). Statin users had a significantly lower hazard of an ICH compared with nonusers (adjusted HR, 0.13; 95% CI, 0.05-0.34). There was no association of CMB and antiplatelet, anticoagulant, or statin use in adjusted models. Conclusions In this US community-based study, antiplatelet and statin use were associated with lower ICH hazard, whereas no association was noted between CMBs and antiplatelets, anticoagulants, and statins. Further study is needed to understand the differential roles of these medications in cerebral microhemorrhages and macrohemorrhages.
抗血小板药物、抗凝药物和他汀类药物常用于多种适应证。这些药物与脑出血(ICH)和脑微出血(CMB)风险之间的关系尚不清楚。
我们对 ARIC(社区动脉粥样硬化风险)研究队列进行了回顾性研究,该队列于 1987 年至 1989 年从美国 4 个社区招募,随访至 2011 年至 2013 年。在此期间,一部分参与者(n=1942)接受了脑磁共振成像检查,以评估 CMB。在基线时未服用某种药物的参与者中,在随后的研究访视中评估了时间变化以及任何抗血小板、抗凝或他汀类药物的使用情况。为了确定药物使用与 ICH 风险和 CMB 比值的关系,分别构建了逻辑和 Cox 比例风险模型,对药物使用的倾向性、其他药物的同时使用以及认知、遗传和影像学数据进行了调整。在长达 20 年的随访期间,共有 15719 名参与者,其中 130 名参与者发生 ICH。与非使用者相比,ICH 前最近一次研究访视时服用抗血小板药物的参与者 ICH 风险显著降低(调整后的危险比[HR],0.53;95%置信区间,0.30-0.92)。与非使用者相比,他汀类药物使用者的 ICH 风险显著降低(调整后的 HR,0.13;95%置信区间,0.05-0.34)。在调整后的模型中,CMB 与抗血小板药物、抗凝药物和他汀类药物之间无相关性。
在这项基于美国社区的研究中,抗血小板药物和他汀类药物的使用与较低的 ICH 风险相关,而 CMB 与抗血小板药物、抗凝药物和他汀类药物之间无相关性。需要进一步研究以了解这些药物在脑微出血和脑大出血中的不同作用。