Department of RadiologyUtah Center for Advanced Imaging Research Salt Lake City UT.
Department of Neurology University of Utah Salt Lake City UT.
J Am Heart Assoc. 2021 Feb;10(5):e019462. doi: 10.1161/JAHA.120.019462. Epub 2021 Feb 15.
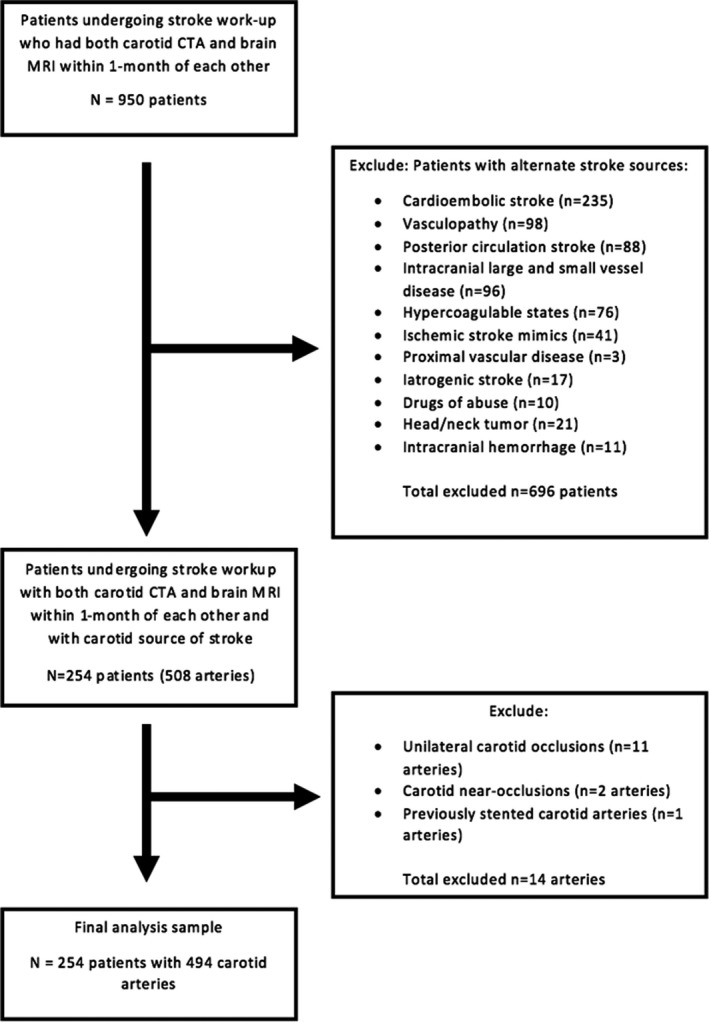
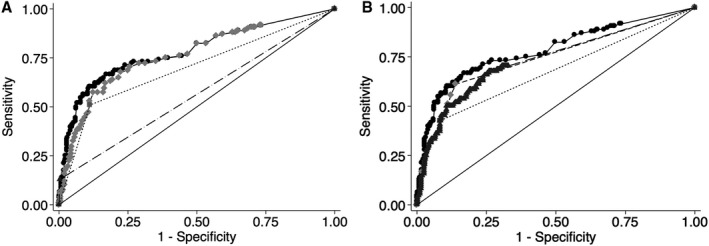
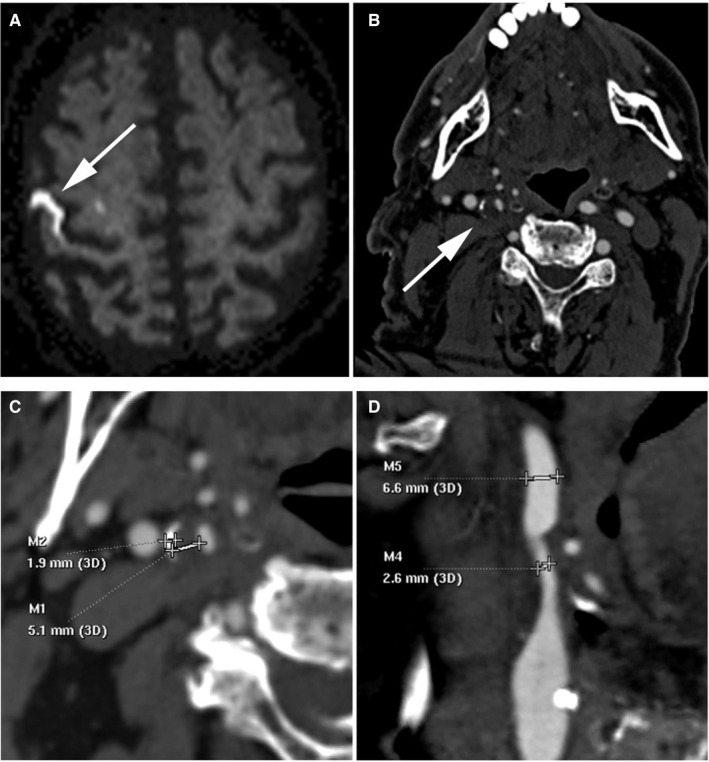
Background Stenosis has historically been the major factor used to determine carotid stroke sources. Recent evidence suggests that specific plaque features detected on imaging may be more highly associated with ischemic stroke than stenosis. We sought to determine computed tomography angiography (CTA) imaging features of carotid plaque that optimally discriminate ipsilateral stroke sources. Methods and Results In this institutional review board-approved retrospective cross-sectional study, 494 ipsilateral carotid CTA-brain magnetic resonance imaging pairs were available for analysis after excluding patients with alternative stroke sources. Carotid CTA and clinical markers were recorded, a multivariable Poisson regression model was fitted, and backward elimination was performed with a 2-sided threshold of <0.10. Discriminatory value was determined using receiver operating characteristic analysis, area under the curve, and bootstrap validation. The final CTA carotid-source stroke prediction model included intraluminal thrombus (prevalence ratio, 2.8 [<0.001]; 95% CI, 1.6-4.9), maximum soft plaque thickness (prevalence ratio, 1.2 [<0.001]; 95% CI, 1.1-1.4), and the rim sign (prevalence ratio, 2.0 [=0.007]; 95% CI, 1.2-3.3). The final discriminatory value (area under the curve=78.3%) was higher than intraluminal thrombus (56.4%, <0.001), maximum soft plaque thickness (76.4%, =0.007), or rim sign alone (69.9%, =0.001). Furthermore, NASCET (North American Symptomatic Carotid Endarterectomy Trial) stenosis categories (cutoffs of 50% and 70%) had lower stroke discrimination (area under the curve=67.4%, <0.001). Conclusions Optimal discrimination of ipsilateral carotid sources of stroke requires information on intraluminal thrombus, maximum soft plaque thickness, and the rim sign. These results argue against the sole use of carotid stenosis to determine stroke sources on CTA, and instead suggest these alternative markers may better diagnose vulnerable carotid plaque and guide treatment decisions.
背景 狭窄一直是决定颈动脉卒中来源的主要因素。最近的证据表明,在影像学上检测到的特定斑块特征与缺血性卒中的相关性可能高于狭窄。我们旨在确定能最佳区分同侧卒中来源的颈动脉斑块 CT 血管造影(CTA)成像特征。
方法和结果 在这项经机构审查委员会批准的回顾性横断面研究中,排除了具有其他卒中来源的患者后,有 494 对同侧颈动脉 CTA-脑部磁共振成像可供分析。记录颈动脉 CTA 和临床标志物,拟合多变量泊松回归模型,并采用双侧阈值<0.10 的向后消除法进行。使用接收者操作特征分析、曲线下面积和引导验证来确定判别值。最终的 CTA 颈动脉源卒中预测模型包括管腔内血栓(患病率比,2.8 [ <0.001];95%CI,1.6-4.9)、最大软斑块厚度(患病率比,1.2 [ <0.001];95%CI,1.1-1.4)和边缘征(患病率比,2.0 [=0.007];95%CI,1.2-3.3)。最终的判别值(曲线下面积=78.3%)高于管腔内血栓(56.4%, <0.001)、最大软斑块厚度(76.4%,=0.007)或边缘征单独(69.9%,=0.001)。此外,NASCET(北美症状性颈动脉内膜切除术试验)狭窄分类(50%和 70%的切点)的卒中判别能力较低(曲线下面积=67.4%, <0.001)。
结论 最佳区分同侧颈动脉卒中来源需要管腔内血栓、最大软斑块厚度和边缘征的信息。这些结果表明,不能仅用颈动脉狭窄来确定 CTA 上的卒中来源,而这些替代标志物可能更好地诊断易损颈动脉斑块并指导治疗决策。