Sun Jie, Canton Gador, Balu Niranjan, Hippe Daniel S, Xu Dongxiang, Liu Jin, Hatsukami Thomas S, Yuan Chun
From the Departments of Radiology (J.S., N.B., D.S.H., D.X., C.Y.), Mechanical Engineering (G.C.), Bioengineering (J.L., C.Y.), and Surgery (T.S.H.), University of Washington, Seattle.
Arterioscler Thromb Vasc Biol. 2016 Apr;36(4):743-9. doi: 10.1161/ATVBAHA.115.307043. Epub 2016 Feb 4.
Effective prevention and management strategies of intraplaque hemorrhage (IPH) remain elusive because of our limited knowledge regarding its contributing factors. This hypothesis-generating study aimed to investigate associations between cardiovascular risk factors and IPH for improved understanding of the pathogenesis of IPH.
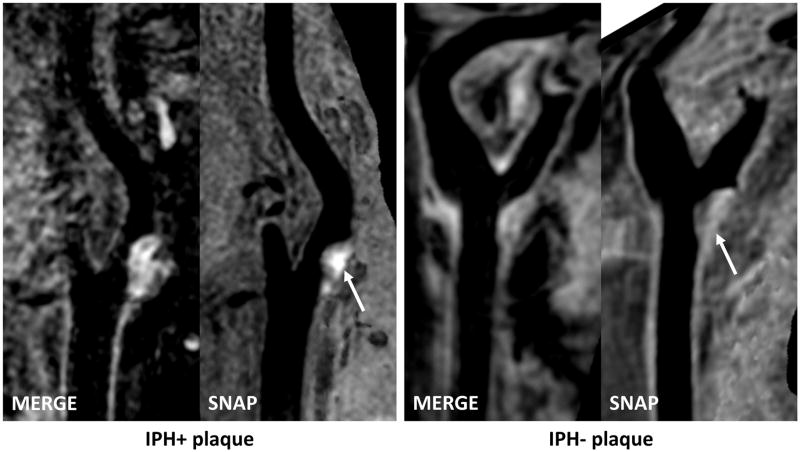
Asymptomatic subjects with 16% to 79% stenosis on ultrasound underwent carotid magnetic resonance imaging using a large-coverage, 3-dimensional magnetic resonance imaging protocol. Individual plaques (maximum thickness >1.5 mm) in bilateral carotid arteries were identified, and presence of IPH was determined. From 80 subjects, 176 de novo plaques were measured, of which 38 (21.6%) contained IPH. Blood pressure (BP), primarily low diastolic BP, was associated with IPH in multivariate analysis adjusted for age, sex, and plaque size (odds ratio with 95% confidence interval per 10-mm Hg increase: 0.51 [0.30-0.88]), which was little changed after adjusting for antihypertensive use and systemic atherosclerosis. Antiplatelet use was associated with IPH in age and sex-adjusted models (P=0.018), for which a trend remained after considering plaque size and past medical history (odds ratio for aspirin alone versus none: 3.1 [0.66-14.8]; odds ratio for clopidogrel or dual therapy versus none: 5.3 [0.80-35.0]; P=0.083).
Low diastolic BP was independently associated with IPH, which was not attributed to treatment difference or BP changes from systemic atherosclerosis. Hemodynamic changes from lowering diastolic BP may be the pathophysiological link. Prospective serial studies are needed to assess whether BP and antiplatelet use are associated with the development of new or repeated IPH.
由于我们对斑块内出血(IPH)的促成因素了解有限,其有效的预防和管理策略仍然难以捉摸。这项产生假设的研究旨在调查心血管危险因素与IPH之间的关联,以更好地理解IPH的发病机制。
对超声显示狭窄程度为16%至79%的无症状受试者,采用大覆盖范围的三维磁共振成像方案进行颈动脉磁共振成像检查。识别双侧颈动脉中的单个斑块(最大厚度>1.5 mm)并确定是否存在IPH。在80名受试者中,共测量了176个新发斑块,其中38个(21.6%)含有IPH。在对年龄、性别和斑块大小进行校正的多变量分析中,血压(BP),主要是低舒张压,与IPH相关(每升高10 mmHg的优势比及95%置信区间:0.51 [0.30 - 0.88]),在校正抗高血压药物使用和全身性动脉粥样硬化后变化不大。在年龄和性别校正模型中,使用抗血小板药物与IPH相关(P = 0.018),在考虑斑块大小和既往病史后这种趋势仍然存在(单独使用阿司匹林与未使用相比的优势比:3.1 [0.66 - 14.8];使用氯吡格雷或双联疗法与未使用相比的优势比:5.3 [0.80 - 35.0];P = 0.083)。
低舒张压与IPH独立相关,这并非归因于治疗差异或全身性动脉粥样硬化导致的血压变化。舒张压降低引起的血流动力学变化可能是其病理生理联系。需要进行前瞻性系列研究来评估血压和抗血小板药物的使用是否与新的或复发性IPH的发生有关。