Department of Epidemiology and Biostatistics, School of Public Health, Imperial College London, St Mary's Hospital, Norfolk Place, London, W21PG, UK.
MRC Centre for Environment and Health, Imperial College, London, UK.
Eur J Epidemiol. 2021 Mar;36(3):299-309. doi: 10.1007/s10654-021-00722-y. Epub 2021 Feb 15.
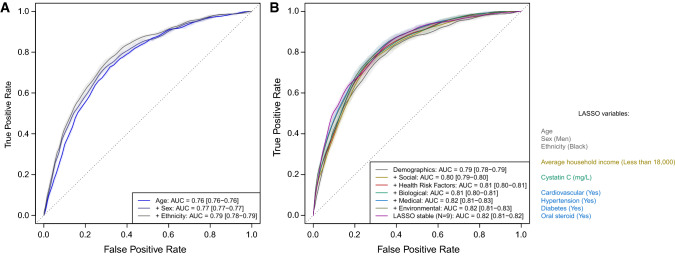
Most studies of severe/fatal COVID-19 risk have used routine/hospitalisation data without detailed pre-morbid characterisation. Using the community-based UK Biobank cohort, we investigate risk factors for COVID-19 mortality in comparison with non-COVID-19 mortality. We investigated demographic, social (education, income, housing, employment), lifestyle (smoking, drinking, body mass index), biological (lipids, cystatin C, vitamin D), medical (comorbidities, medications) and environmental (air pollution) data from UK Biobank (N = 473,550) in relation to 459 COVID-19 and 2626 non-COVID-19 deaths to 21 September 2020. We used univariate, multivariable and penalised regression models. Age (OR = 2.76 [2.18-3.49] per S.D. [8.1 years], p = 2.6 × 10), male sex (OR = 1.47 [1.26-1.73], p = 1.3 × 10) and Black versus White ethnicity (OR = 1.21 [1.12-1.29], p = 3.0 × 10) were independently associated with and jointly explanatory of (area under receiver operating characteristic curve, AUC = 0.79) increased risk of COVID-19 mortality. In multivariable regression, alongside demographic covariates, being a healthcare worker, current smoker, having cardiovascular disease, hypertension, diabetes, autoimmune disease, and oral steroid use at enrolment were independently associated with COVID-19 mortality. Penalised regression models selected income, cardiovascular disease, hypertension, diabetes, cystatin C, and oral steroid use as jointly contributing to COVID-19 mortality risk; Black ethnicity, hypertension and oral steroid use contributed to COVID-19 but not non-COVID-19 mortality. Age, male sex and Black ethnicity, as well as comorbidities and oral steroid use at enrolment were associated with increased risk of COVID-19 death. Our results suggest that previously reported associations of COVID-19 mortality with body mass index, low vitamin D, air pollutants, renin-angiotensin-aldosterone system inhibitors may be explained by the aforementioned factors.
大多数关于严重/致命 COVID-19 风险的研究都使用常规/住院数据,而没有详细的发病前特征描述。我们利用基于社区的英国生物库队列,研究了 COVID-19 死亡率与非 COVID-19 死亡率的风险因素。我们调查了英国生物库中的人口统计学、社会(教育、收入、住房、就业)、生活方式(吸烟、饮酒、体重指数)、生物学(脂质、胱抑素 C、维生素 D)、医疗(合并症、药物)和环境(空气污染)数据,这些数据与 2020 年 9 月 21 日之前的 459 例 COVID-19 和 2626 例非 COVID-19 死亡有关。我们使用了单变量、多变量和惩罚回归模型。年龄(每标准差增加 8.1 岁,OR=2.76 [2.18-3.49],p=2.6×10)、男性(OR=1.47 [1.26-1.73],p=1.3×10)和黑人相对于白人种族(OR=1.21 [1.12-1.29],p=3.0×10)与 COVID-19 死亡率的增加独立相关,并共同解释了(ROC 曲线下面积,AUC=0.79)。在多变量回归中,除了人口统计学协变量外,医护人员、当前吸烟者、患有心血管疾病、高血压、糖尿病、自身免疫性疾病以及登记时使用口服类固醇,这些因素与 COVID-19 死亡率独立相关。惩罚回归模型选择收入、心血管疾病、高血压、糖尿病、胱抑素 C 和口服类固醇的使用作为 COVID-19 死亡率风险的共同贡献因素;黑人种族、高血压和口服类固醇的使用与 COVID-19 相关,但与非 COVID-19 无关。年龄、男性和黑人种族,以及登记时的合并症和口服类固醇的使用,与 COVID-19 死亡风险的增加相关。我们的结果表明,以前报道的 COVID-19 死亡率与体重指数、低维生素 D、空气污染物、肾素-血管紧张素-醛固酮系统抑制剂之间的关联可能可以用上述因素来解释。