Clinical Division and Laboratory of Intensive Care Medicine, Department of Cellular and Molecular Medicine, KU Leuven, Herestraat 49, 3000, Leuven, Belgium.
Medical Intensive Care Unit, Department of General Internal Medicine, UZ Leuven, Leuven, Belgium.
Intensive Care Med. 2018 Dec;44(12):2048-2058. doi: 10.1007/s00134-018-5427-y. Epub 2018 Oct 29.
Low plasma ACTH in critically ill patients may be explained by shock/inflammation-induced hypothalamus-pituitary damage or by feedback inhibition exerted by elevated plasma free cortisol. One can expect augmented/prolonged ACTH-responses to CRH injection with hypothalamic damage, immediately suppressed responses with pituitary damage, and delayed decreased responses in prolonged critical illness with feedback inhibition.
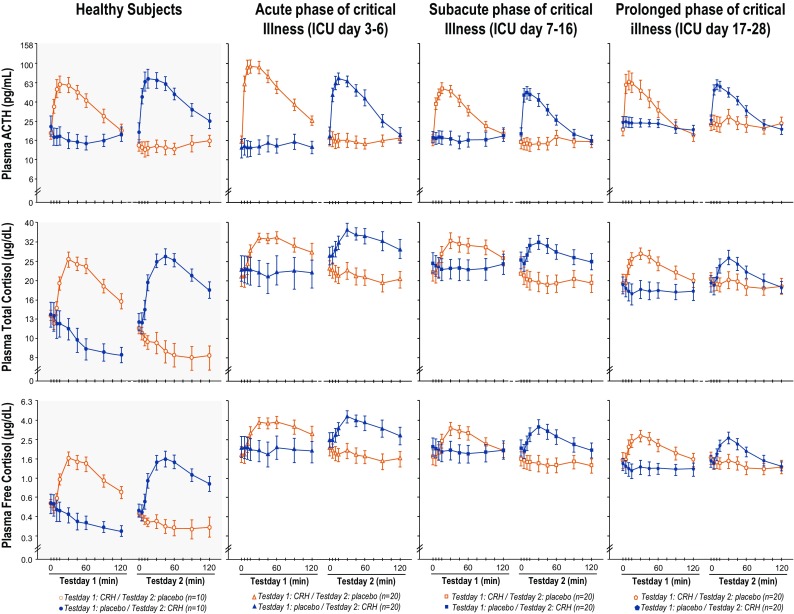
This randomized, double-blind, placebo-controlled crossover cohort study, compared ACTH responses to 100 µg IV CRH and placebo in 3 cohorts of 40 matched patients in the acute (ICU-day 3-6), subacute (ICU-day 7-16) or prolonged phase (ICU-day 17-28) of critical illness, with 20 demographically matched healthy subjects. CRH or placebo was injected in random order on two consecutive days. Blood was sampled repeatedly over 135 min and AUC responses to placebo were subtracted from those to CRH.
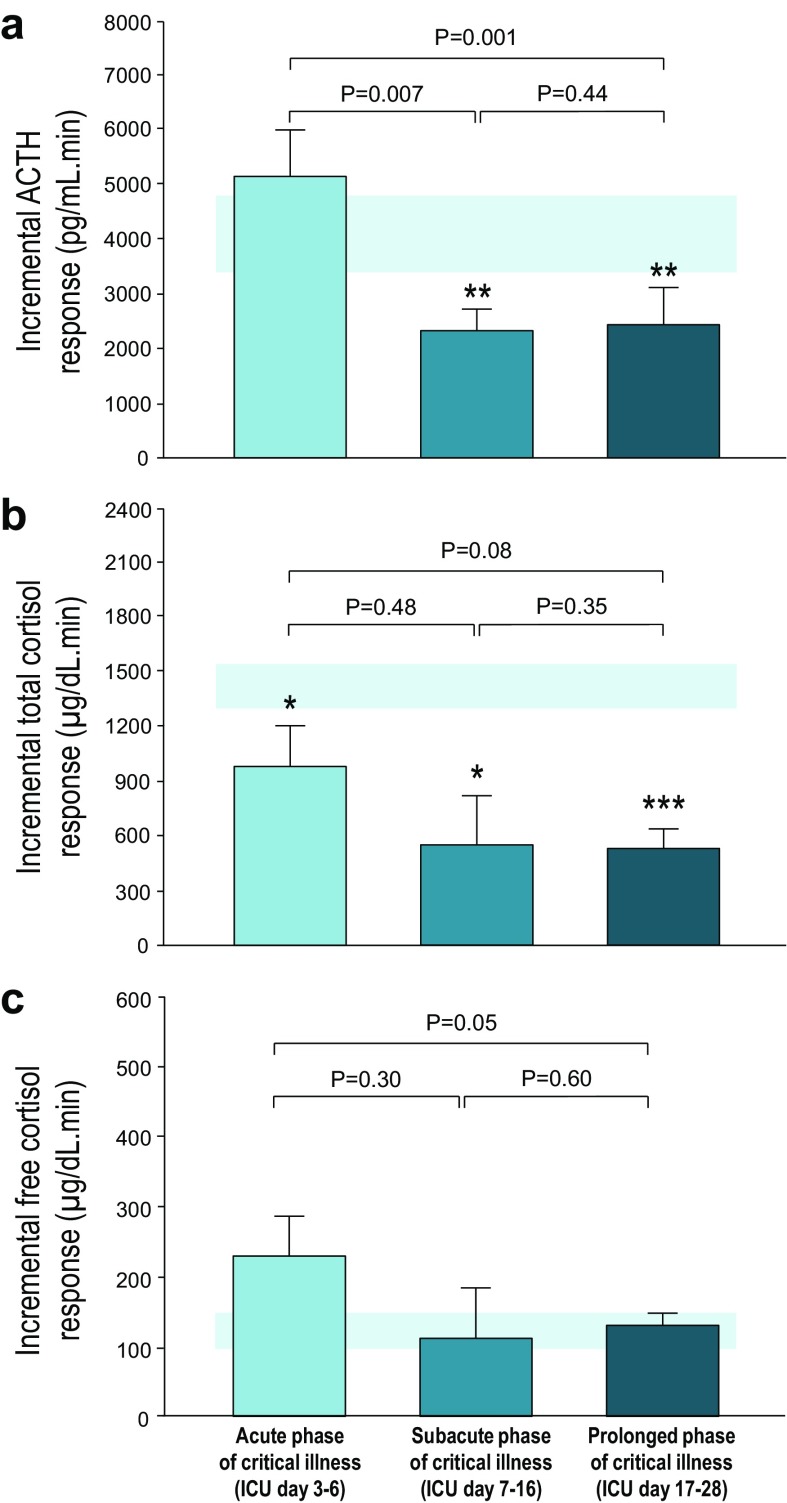
Patients had normal mean ± SEM plasma ACTH concentrations (25.5 ± 1.6 versus 24.8 ± 3.6 pg/ml in healthy subjects, P = 0.54) but elevated free cortisol concentrations (3.11 ± 0.27 versus 0.58 ± 0.05 µg/dl in healthy subjects, P < 0.0001). The order of the CRH/placebo injections did not affect the ACTH responses, hence results were pooled. Patients in the acute phase of illness had normal mean ± SEM ACTH responses (5149 ± 848 pg/mL min versus 4120 ± 688 pg/mL min in healthy subjects; P = 0.77), whereas those in the subacute (2333 ± 387 pg/mL min, P = 0.01) and prolonged phases (2441 ± 685 pg/mL min, P = 0.001) were low, irrespective of sepsis/septic shock or risk of death.
Suppressed ACTH responses to CRH in the more prolonged phases, but not acute phase, of critical illness are compatible with feedback inhibition exerted by elevated free cortisol, rather than by cellular damage to hypothalamus and/or pituitary.
危重病患者低血浆 ACTH 可能是由休克/炎症引起的下丘脑-垂体损伤引起的,也可能是由升高的血浆游离皮质醇引起的反馈抑制引起的。人们可以预期,在下丘脑损伤时,CRH 注射后的 ACTH 反应会增强/延长,垂体损伤时反应会立即受到抑制,而在长时间的危重病期间反馈抑制时,反应会延迟减少。
这项随机、双盲、安慰剂对照的交叉队列研究,比较了 3 组 40 例匹配患者(急性组[ICU 第 3-6 天]、亚急性组[ICU 第 7-16 天]或慢性期[ICU 第 17-28 天])在急性(ICU 第 3-6 天)、亚急性(ICU 第 7-16 天)或慢性期(ICU 第 17-28 天)中对 100µg IV CRH 和安慰剂的 ACTH 反应,每组 40 例,并与 20 名年龄匹配的健康受试者进行了比较。CRH 或安慰剂以随机顺序连续两天注射。在 135 分钟内多次取样,并从 CRH 的反应中减去安慰剂的 AUC 反应。
患者的平均 ACTH 浓度(25.5±1.6 pg/ml 与健康受试者的 24.8±3.6 pg/ml,P=0.54)正常,但游离皮质醇浓度升高(3.11±0.27 µg/dl 与健康受试者的 0.58±0.05 µg/dl,P<0.0001)。CRH/安慰剂注射的顺序不影响 ACTH 反应,因此结果被汇总。急性疾病患者的平均 ACTH 反应正常(5149±848 pg/ml·min 与健康受试者的 4120±688 pg/ml·min;P=0.77),而亚急性(2333±387 pg/ml·min,P=0.01)和慢性期(2441±685 pg/ml·min,P=0.001)患者的反应较低,无论是否存在脓毒症/脓毒性休克或死亡风险。
在危重病的更长阶段而不是急性期,CRH 对 ACTH 的反应受到抑制,这与升高的游离皮质醇引起的反馈抑制一致,而不是与下丘脑和/或垂体的细胞损伤一致。