Division of Molecular Imaging and Neuropathology (Mann, Michel) and Division of Child and Adolescent Psychiatry (Auerbach), New York State Psychiatric Institute and Department of Psychiatry, Columbia University, New York (Mann, Auerbach); Division of Clinical Developmental Neuroscience, Sackler Institute for Developmental Psychobiology, Columbia University, New York (Auerbach).
Am J Psychiatry. 2021 Jul;178(7):611-624. doi: 10.1176/appi.ajp.2020.20060864. Epub 2021 Feb 18.
The authors sought to identify scalable evidence-based suicide prevention strategies.
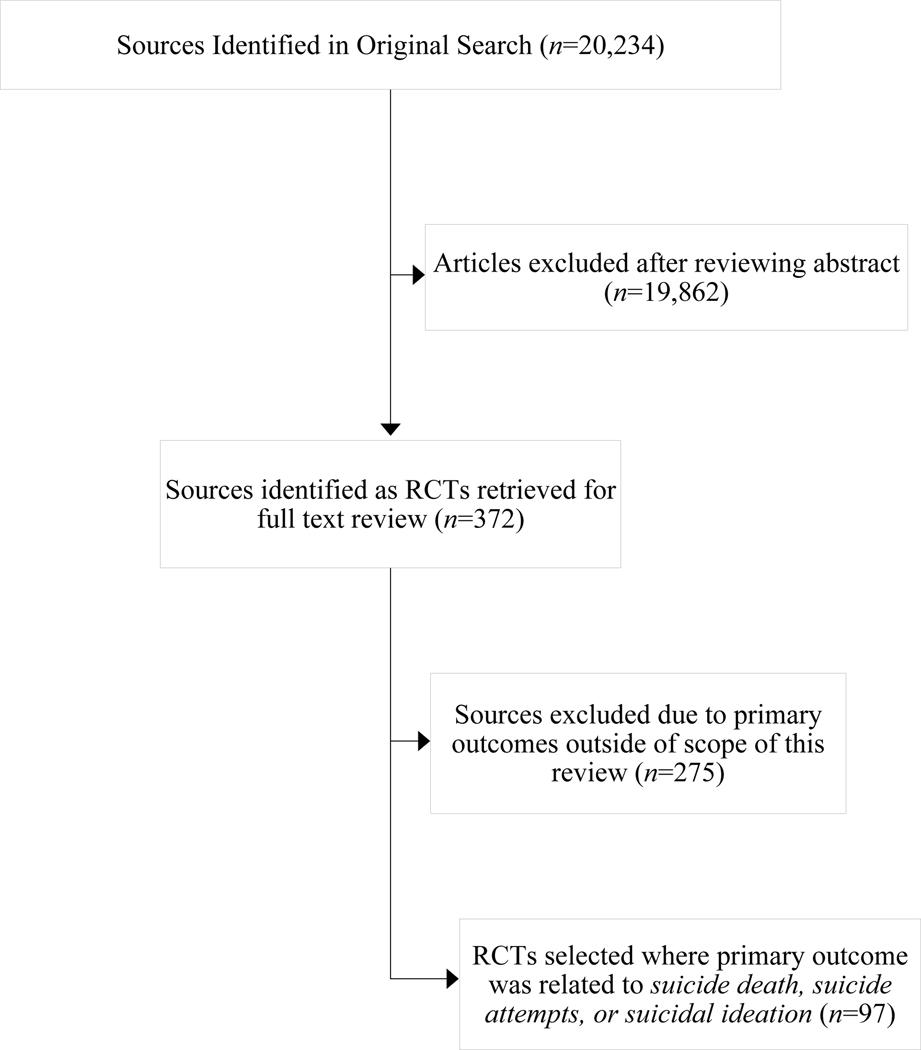
A search of PubMed and Google Scholar identified 20,234 articles published between September 2005 and December 2019, of which 97 were randomized controlled trials with suicidal behavior or ideation as primary outcomes or epidemiological studies of limiting access to lethal means, using educational approaches, and the impact of antidepressant treatment.
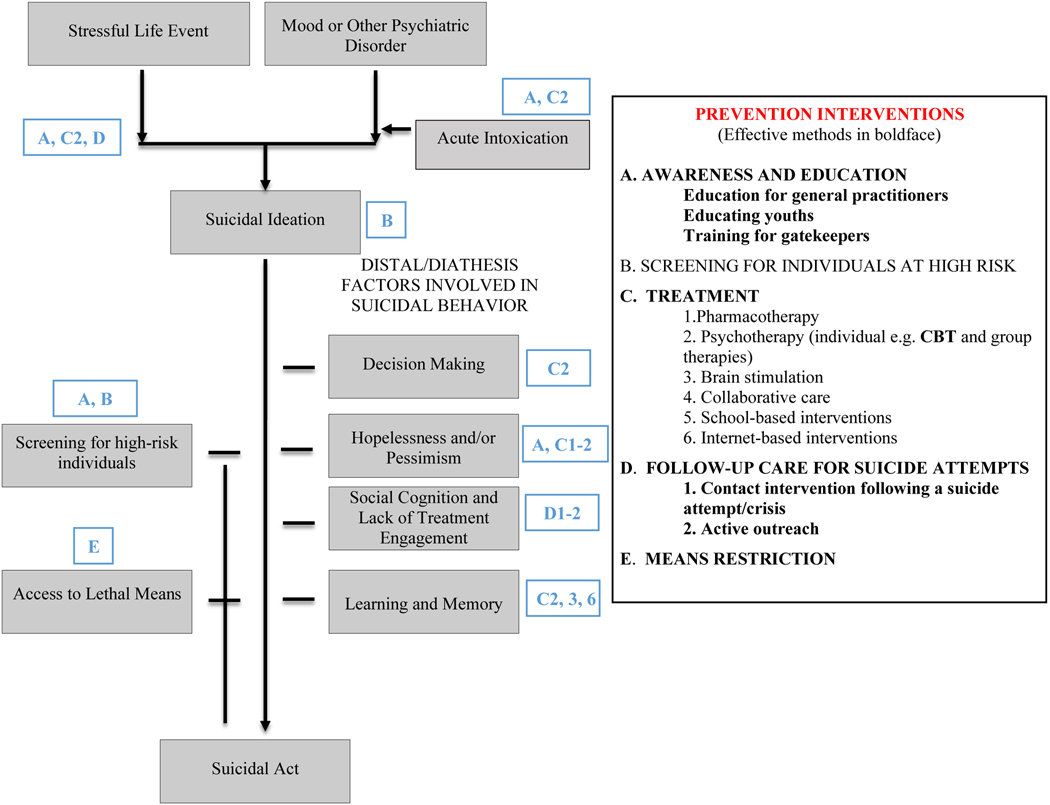
Training primary care physicians in depression recognition and treatment prevents suicide. Educating youths on depression and suicidal behavior, as well as active outreach to psychiatric patients after discharge or a suicidal crisis, prevents suicidal behavior. Meta-analyses find that antidepressants prevent suicide attempts, but individual randomized controlled trials appear to be underpowered. Ketamine reduces suicidal ideation in hours but is untested for suicidal behavior prevention. Cognitive-behavioral therapy and dialectical behavior therapy prevent suicidal behavior. Active screening for suicidal ideation or behavior is not proven to be better than just screening for depression. Education of gatekeepers about youth suicidal behavior lacks effectiveness. No randomized trials have been reported for gatekeeper training for prevention of adult suicidal behavior. Algorithm-driven electronic health record screening, Internet-based screening, and smartphone passive monitoring to identify high-risk patients are understudied. Means restriction, including of firearms, prevents suicide but is sporadically employed in the United States, even though firearms are used in half of all U.S. suicides.
Training general practitioners warrants wider implementation and testing in other nonpsychiatrist physician settings. Active follow-up of patients after discharge or a suicide-related crisis should be routine, and restricting firearm access by at-risk individuals warrants wider use. Combination approaches in health care systems show promise in reducing suicide in several countries, but evaluating the benefit attributable to each component is essential. Further suicide rate reduction requires evaluating newer approaches, such as electronic health record-derived algorithms, Internet-based screening methods, ketamine's potential benefit for preventing attempts, and passive monitoring of acute suicide risk change.
作者试图确定可扩展的基于证据的自杀预防策略。
在 PubMed 和 Google Scholar 中搜索,确定了 20234 篇发表于 2005 年 9 月至 2019 年 12 月间的文章,其中 97 项为以自杀行为或意念为主要结局的随机对照试验,或为限制获取致命手段、采用教育方法,以及抗抑郁治疗影响的流行病学研究。
培训初级保健医生识别和治疗抑郁症可预防自杀。对青少年进行抑郁症和自杀行为教育,以及在出院或自杀危机后主动接触精神科患者,可预防自杀行为。荟萃分析发现,抗抑郁药可预防自杀企图,但个别随机对照试验的效力似乎不足。氯胺酮可在数小时内减少自杀意念,但尚未经过预防自杀行为的测试。认知行为疗法和辩证行为疗法可预防自杀行为。主动筛查自杀意念或行为并不比仅仅筛查抑郁更有效。关于青少年自杀行为的教育对预防成人自杀行为缺乏有效性。尚未报告针对预防成人自杀行为的守门人培训的随机试验。基于算法的电子健康记录筛查、基于互联网的筛查以及用于识别高危患者的智能手机被动监测研究较少。限制手段,包括限制枪支,可预防自杀,但在美国零星使用,尽管枪支在美国一半的自杀事件中被使用。
培训全科医生值得在其他非精神科医生环境中更广泛地实施和测试。在出院或与自杀相关的危机后,对患者进行积极的随访应成为常规,限制高危个体获取枪支应更广泛地使用。在一些国家,医疗系统中的综合方法在降低自杀率方面显示出了前景,但评估每种方法的获益至关重要。进一步降低自杀率需要评估新方法,如基于电子健康记录的算法、基于互联网的筛查方法、氯胺酮预防尝试的潜在益处以及急性自杀风险变化的被动监测。