van Eekelen R, Rosielle K, van Welie N, Dreyer K, van Wely M, Mol B W, Eijkemans M J, Mijatovic V, van Geloven N
Amsterdam UMC, Academic Medical Centre, Centre for Reproductive Medicine, Amsterdam, the Netherlands.
Department of Reproductive Medicine, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, the Netherlands.
Hum Reprod Open. 2020 Nov 17;2020(4):hoaa047. doi: 10.1093/hropen/hoaa047. eCollection 2020.
Can we replicate the finding that the benefit of IUI-ovarian stimulation (IUI-OS) compared to expectant management for couples with unexplained subfertility depends on the prognosis of natural conception?
The estimated benefit of IUI-OS did not depend on the prognosis of natural conception but did depend on when treatment was started after diagnosis, with starting IUI-OS later yielding a larger absolute and relative benefit of treatment.
IUI-OS is often the first-line treatment for couples with unexplained subfertility. Two randomized controlled trials (RCTs) compared IUI-OS to expectant management using different thresholds for the prognosis of natural conception as inclusion criteria and found different results. In a previous study (a Dutch national cohort), it was found that the benefit of IUI-OS compared to expectant management seemed dependent on the prognosis of natural conception, but this finding warrants replication.
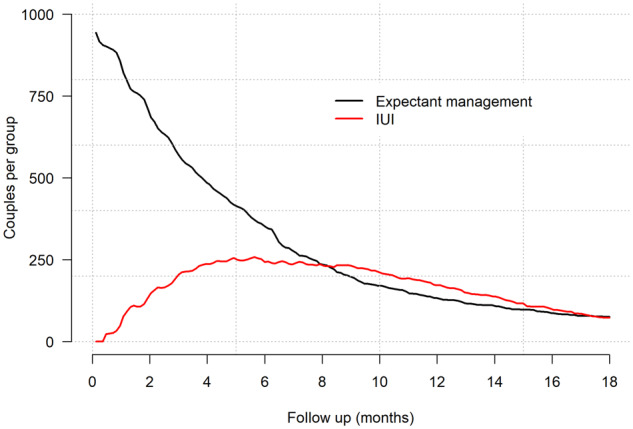
We conducted a secondary analysis of the H2Oil study (n = 1119), a multicentre RCT that evaluated the effect of oil-based contrast versus water-based contrast during hysterosalpingography (HSG). Couples were randomized before HSG and followed up for 3-5 years. We selected couples with unexplained subfertility who received HSG and had follow-up or pregnancy data available. Follow-up was censored at the start of IVF, after the last IUI cycle or at last contact and was truncated at a maximum of 18 months after the fertility workup.
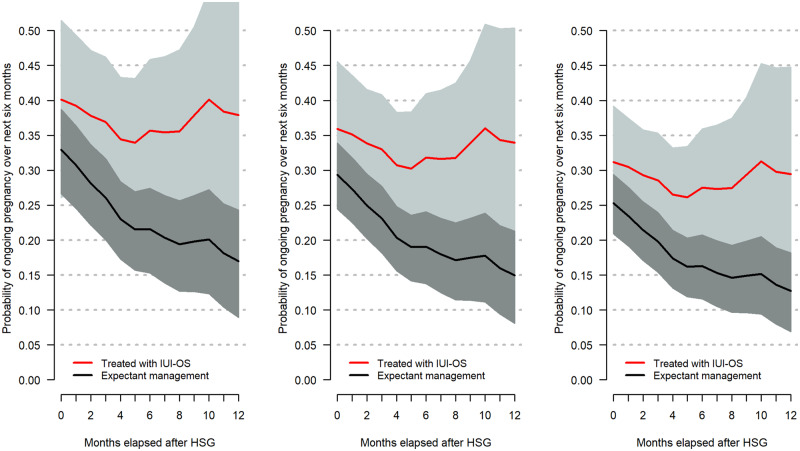
PARTICIPANTS/MATERIALS SETTING METHODS: The endpoint was time to conception leading to an ongoing pregnancy. We used the sequential Cox approach comparing in each month the ongoing pregnancy rates over the next 6 months of couples who started IUI-OS to couples who did not. We calculated the prognosis of natural conception for individual couples, updated this over consecutive failed cycles and evaluated whether prognosis modified the effect of starting IUI-OS. We corrected for known predictors of conception using inverse probability weighting.
Data from 975 couples were available. There were 587 couples who received at least one IUI-OS cycle within 18 months after HSG of whom 221 conceived leading to an ongoing pregnancy (rate: 0.74 per couple per year over a median follow-up for IUI of 5 months). The median period between HSG and starting IUI-OS was 4 months. Out of 388 untreated couples, 299 conceived naturally (rate: 0.56 per couple per year over a median follow-up of 4 months). After creating our mimicked trial datasets, starting IUI-OS was associated with a higher chance of ongoing pregnancy by a pooled, overall hazard ratio of 1.50 (95% CI: 1.19-1.89) compared to expectant management. We did not find strong evidence that the effect of treatment was modified by a couple's prognosis of achieving natural conception (Akaike's Information Criterion (AIC) decreased by 1 point). The effect of treatment was dependent on when couples started IUI-OS (AIC decreased by more than 2 points). The patterns of estimated absolute chances over time for couples with increasingly better prognoses were different from the previous study but the finding that starting later yields a larger benefit of treatment was similar. We found IUI-OS increased the absolute chance of pregnancy by at least 5% compared to expectant management. The absolute chance of pregnancy after IUI-OS seems less variable between couples and starting times of treatment than the absolute chance after expectant management.
This is a secondary analysis, as the H2Oil trial was not designed with this research question in mind. Owing to sample size restrictions, it remained difficult to distinguish between the ranges of prognoses in which true benefit was found.
We replicated the finding that starting IUI-OS later after diagnosis yields a larger absolute and relative benefit of treatment. We did not replicate the dependency of the effect of IUI-OS on the prognosis of natural conception and could not identify clear thresholds for the prognosis of natural conception when IUI-OS was and/or was not effective. Because many of these couples still have good chances of natural conception at the time of diagnosis, we suggest clinicians should advise couples to delay the start of IUI-OS for several months to avoid unnecessary treatment.
STUDY FUNDING/COMPETING INTERESTS: The H2Oil study (NTR 3270) was an investigator-initiated study that was funded by the two academic institutions (AMC and VUmc) of the Amsterdam UMC. The follow-up study (NTR 6577) was also an investigator-initiated study with funding by Guerbet, France. The funders had no role in study design, collection, analysis and interpretation of the data. B.W.M. is supported by an Investigator grant (GNT1176437) from the Australian National Health and Medical Research Council (NHMRC). K.D. reports receiving travel and speaker fees from Guerbet. B.W.M. reports consultancy for ObsEva, Merck, Merck KGaA, iGenomix and Guerbet. V.M. reports receiving travel- and speaker fees as well as research grants from Guerbet.
对于不明原因的不育夫妇,与期待治疗相比,宫腔内人工授精联合卵巢刺激(IUI-OS)的益处是否取决于自然受孕的预后,这一发现能否被复制?
IUI-OS的估计益处并不取决于自然受孕的预后,而是取决于诊断后何时开始治疗,延迟开始IUI-OS会产生更大的绝对和相对治疗益处。
IUI-OS通常是不明原因不育夫妇的一线治疗方法。两项随机对照试验(RCT)将IUI-OS与期待治疗进行比较,使用不同的自然受孕预后阈值作为纳入标准,结果不同。在之前的一项研究(荷兰全国队列研究)中,发现与期待治疗相比,IUI-OS的益处似乎取决于自然受孕的预后,但这一发现需要复制。
研究设计、规模、持续时间:我们对H2Oil研究(n = 1119)进行了二次分析,这是一项多中心RCT,评估了子宫输卵管造影术(HSG)期间油基造影剂与水基造影剂的效果。夫妇在HSG前被随机分组,并随访3至5年。我们选择了接受HSG且有随访或妊娠数据的不明原因不育夫妇。随访在体外受精开始时、最后一个IUI周期后或最后一次接触时进行截尾,在生育检查后最多18个月进行截断。
参与者/材料、设置、方法:终点是导致持续妊娠的受孕时间。我们采用序贯Cox方法,每月比较开始IUI-OS的夫妇与未开始IUI-OS的夫妇在接下来6个月内的持续妊娠率。我们计算了个体夫妇自然受孕的预后,在连续失败周期中更新,并评估预后是否改变开始IUI-OS的效果。我们使用逆概率加权法校正已知的受孕预测因素。
可获得975对夫妇的数据。有587对夫妇在HSG后18个月内接受了至少一个IUI-OS周期,其中221对受孕并导致持续妊娠(率:在IUI的中位随访5个月期间,每对夫妇每年0.74)。HSG与开始IUI-OS之间的中位时间为4个月。在388对未治疗的夫妇中,299对自然受孕(率:在中位随访4个月期间,每对夫妇每年0.56)。在创建模拟试验数据集后,与期待治疗相比,开始IUI-OS与更高的持续妊娠机会相关,汇总的总体风险比为1.50(95%CI:1.19 - 1.89)。我们没有发现有力证据表明治疗效果因夫妇自然受孕的预后而改变(赤池信息准则(AIC)降低1分)。治疗效果取决于夫妇开始IUI-OS的时间(AIC降低超过2分)。随着预后越来越好的夫妇,估计的绝对机会随时间变化的模式与之前的研究不同,但延迟开始治疗会产生更大治疗益处这一发现是相似的。我们发现与期待治疗相比,IUI-OS使妊娠的绝对机会增加了至少5%。IUI-OS后妊娠的绝对机会在夫妇和治疗开始时间之间的变化似乎比期待治疗后的绝对机会更小。
局限性、谨慎理由:这是一项二次分析,因为H2Oil试验并非针对该研究问题设计。由于样本量限制,仍然难以区分发现真正益处的预后范围。
我们复制了诊断后延迟开始IUI-OS会产生更大的绝对和相对治疗益处这一发现。我们没有复制IUI-OS效果对自然受孕预后的依赖性,并且无法确定IUI-OS有效和/或无效时自然受孕预后的明确阈值。因为这些夫妇中的许多人在诊断时仍有良好的自然受孕机会,我们建议临床医生应建议夫妇将IUI-OS的开始时间推迟几个月,以避免不必要的治疗。
研究资金/利益冲突:H2Oil研究(NTR 3270)是一项由研究者发起的研究,由阿姆斯特丹大学医学中心的两个学术机构(AMC和VUmc)资助。随访研究(NTR 6577)也是一项由研究者发起的研究,由法国Guerbet资助。资助者在研究设计、数据收集、分析和解释中没有作用。B.W.M.得到了澳大利亚国家卫生与医学研究委员会(NHMRC)的研究者资助(GNT1176437)。K.D.报告从Guerbet获得旅行和演讲费用。B.W.M.报告为ObsEva、默克、默克集团、iGenomix和Guerbet提供咨询服务。V.M.报告从Guerbet获得旅行和演讲费用以及研究资助。