Jandial Aditya, Mishra Kundan, Sandal Rajeev, Kant Sahu Kamal
Department of Internal Medicine (Adult Clinical Hematology Division), Postgraduate Institute of Medical Education and Research, Chandigarh (Union Territory), India.
Department of Clinical Hematology and Stem Cell Transplant, Army Hospital (Research & Referral) New Delhi, India.
Ther Adv Infect Dis. 2021 Feb 3;8:2049936121991377. doi: 10.1177/2049936121991377. eCollection 2021 Jan-Dec.
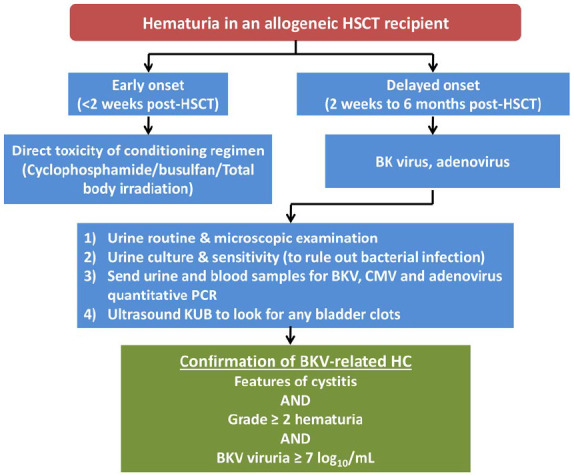
BK virus (BKV)-related haemorrhagic cystitis (HC) is an important cause of morbidity following allogeneic haematopoietic stem cell transplantation (HSCT). The various risk factors include high-level BKV viruria and/or viremia, myeloablative conditioning, acute graft host disease (GVHD), cytomegalovirus viremia, and unrelated or HLA-mismatched donor. The presence of high plasma BK viral load and cytopenias have been implicated as important predictors for protracted disease course. These patients frequently require hospitalisation which may extend for several weeks. Supportive measures in the form of analgesics, intravenous hydration, bladder irrigation, and transfusion support remain the mainstay of management. Various drugs have been used with limited success in this setting. These include antiviral drugs, fluoroquinolones, leflunomide, growth factors, clotting factors, estrogens, and prostaglandins. The role of adoptive cellular immunotherapy has also been explored but lacks clinical validation. The strategies aimed at expediting urothelial repair like hyperbaric oxygen therapy (HBOT), intravesical fibrin glue and platelet-rich plasma (PRP) are emerging. Some patients with severe disease do require surgical intervention to relieve urinary obstruction. The frequent co-occurrence of acute GVHD and CMV disease further complicates the management in such patients. There is an unmet need for effective and evidence-based options for the prevention and management of this disease. Due to lack of robust data supported by randomised trials, the acceptability of the available guidelines to simplify the treatment is expected to be low. Despite the availability of various treatment options, the management of BKV-related HC in day-to-day practice continues to be a challenge. The aim of this article is to put forward an up-to-date review of the preventive and therapeutic strategies for BKV-related HC.
BK病毒(BKV)相关的出血性膀胱炎(HC)是异基因造血干细胞移植(HSCT)后发病的重要原因。各种风险因素包括高水平的BKV病毒尿和/或病毒血症、清髓性预处理、急性移植物抗宿主病(GVHD)、巨细胞病毒病毒血症以及无关或HLA不匹配的供体。高血浆BK病毒载量和血细胞减少症的存在被认为是疾病病程迁延的重要预测指标。这些患者经常需要住院,住院时间可能长达数周。以镇痛药、静脉补液、膀胱冲洗和输血支持等形式的支持性措施仍然是治疗的主要手段。在这种情况下,各种药物的使用效果有限。这些药物包括抗病毒药物、氟喹诺酮类、来氟米特、生长因子、凝血因子、雌激素和前列腺素。过继性细胞免疫疗法的作用也已得到探索,但缺乏临床验证。旨在加速尿路上皮修复的策略,如高压氧治疗(HBOT)、膀胱内注射纤维蛋白胶和富含血小板血浆(PRP)正在兴起。一些重症患者确实需要手术干预以缓解尿路梗阻。急性GVHD和CMV疾病的频繁并发进一步使这类患者的治疗复杂化。对于这种疾病的预防和管理,迫切需要有效且基于证据的选择。由于缺乏随机试验支持的有力数据,现有简化治疗指南的可接受性预计较低。尽管有各种治疗选择,但在日常实践中,BKV相关HC的管理仍然是一项挑战。本文的目的是对BKV相关HC的预防和治疗策略进行最新综述。