Furushima Kozo, Funakoshi Tadanao, Kusano Hiroshi, Miyamoto Azusa, Takahashi Toru, Horiuchi Yukio, Itoh Yoshiyasu
Keiyu Orthopaedic Hospital, Tatebayashi, Japan.
Arthrosc Sports Med Rehabil. 2021 Jan 30;3(1):e155-e162. doi: 10.1016/j.asmr.2020.08.019. eCollection 2021 Feb.
To assess the feasibility, safety, and clinical outcomes of an endoscopic-assisted transaxillary approach of first rib resection for thoracic outlet syndrome (TOS) and to compare the differences in demographic and clinical data between satisfactory and unsatisfactory outcomes using this approach.
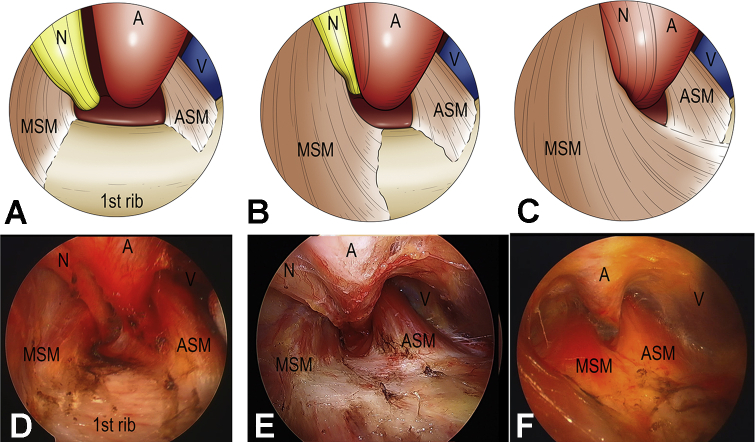
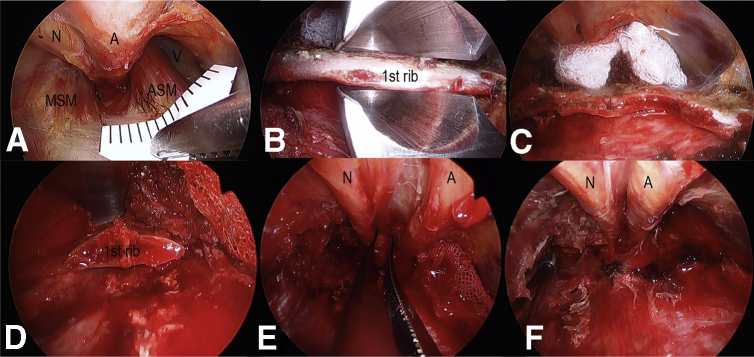
We retrospectively identified patients who underwent endoscopic-assisted first rib partial resection. A transaxillary approach for the first rib resection and neurovascular decompression were undertaken under magnified visualization. Endoscopic classification of neurovascular bundle (NVB) patterns and interscalene distance (ISD) between anterior and middle scalene muscles were evaluated intraoperatively. We assessed the Roos and DASH scores.
We reviewed 131 cases of TOS (48 women and 83 men; mean age 26.2 years; range 12 to 57). Roos classification revealed 80.2% excellent or good results. DASH scores improved significantly from 40.7 ± 20.0 to 15.7 ± 19.6 ( < .001). The complication rate was low (5.3%), with 4 pneumothorax and 3 other complications. Intraoperative NVB classification revealed 30 cases of parallel type, in which the artery and nerve travel in parallel; 69 oblique types, and 30 vertical types, in which the nerve was completely behind the middle scalene muscle or abnormal band. The ISD was narrower (5.4 ± 3.6 mm) than in previous cadaveric studies. The ISD in the parallel patterns was wider than that in the vertical patterns. In the satisfactory group, we found a significantly larger number of men, younger patients, athletes, and patients with a lower preoperative DASH score.
An endoscopic-assisted transaxillary approach for first rib resection in TOS provides an excellent magnified visualization, safely allowing sufficient decompression of the neurovascular bundle and satisfactory surgical outcomes. Younger male athletes with TOS may be better candidates for this procedure.
IV, therapeutic case series.
评估内镜辅助经腋窝入路第一肋切除术治疗胸廓出口综合征(TOS)的可行性、安全性和临床疗效,并比较采用该方法获得满意和不满意疗效的患者在人口统计学和临床数据方面的差异。
我们回顾性纳入了接受内镜辅助第一肋部分切除术的患者。在放大视野下采用经腋窝入路进行第一肋切除和神经血管减压。术中评估神经血管束(NVB)模式的内镜分类以及前、中斜角肌之间的斜角肌间隙距离(ISD)。我们评估了Roos和DASH评分。
我们回顾了131例TOS患者(48例女性和83例男性;平均年龄26.2岁;范围12至57岁)。Roos分类显示80.2%的结果为优或良。DASH评分从40.7±20.0显著改善至15.7±19.6(P<.001)。并发症发生率较低(5.3%),包括4例气胸和3例其他并发症。术中NVB分类显示30例平行型,即动脉和神经并行;69例斜行型,30例垂直型,即神经完全位于中斜角肌后方或存在异常束带。ISD比以往尸体研究中的更窄(5.4±3.6mm)。平行型的ISD比垂直型更宽。在满意组中,我们发现男性、年轻患者、运动员以及术前DASH评分较低的患者数量显著更多。
内镜辅助经腋窝入路治疗TOS的第一肋切除术提供了出色的放大视野,能够安全地实现神经血管束的充分减压并获得满意的手术效果。患有TOS的年轻男性运动员可能是该手术的更好候选者。
IV,治疗性病例系列。