Wu Ya-Hua, Lin Ming-Qiang, Wang Zhi-Ping, Li Jian-Cheng
Department of Radiation Oncology, Fujian Cancer Hospital and Fujian Medical University Cancer Hospital, Fuzhou 350014, China.
Transl Oncol. 2021 May;14(5):101037. doi: 10.1016/j.tranon.2021.101037. Epub 2021 Feb 19.
Nowadays, there were few studies reporting the risk stratification of patients with esophageal squamous cell carcinoma (ESCC) after neoadjuvant chemoradiation (NCRT) and surgery. We aimed to establish a simple risk stratification to help postoperative detection and adjuvant treatment.
We included 146 patients with locally advanced ESCC who received NCRT followed by esophagectomy. The impacts of clinicopathological factors on overall survival (OS) and disease-free survival (DFS) were analyzed. The recurrence site, time, and frequency were recorded as well.
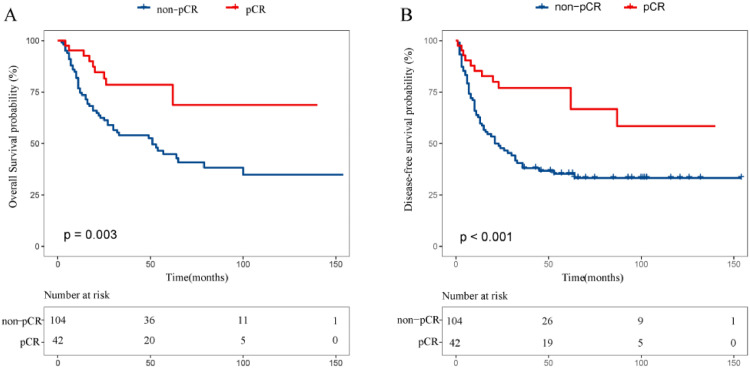
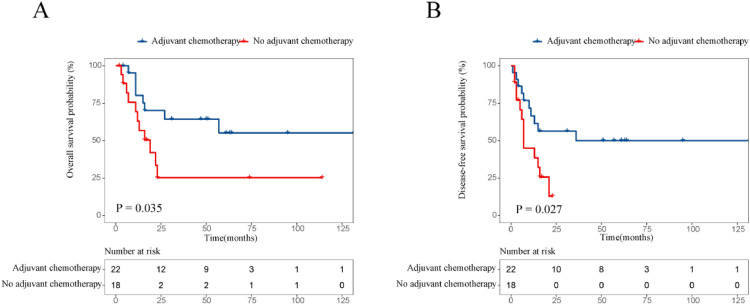
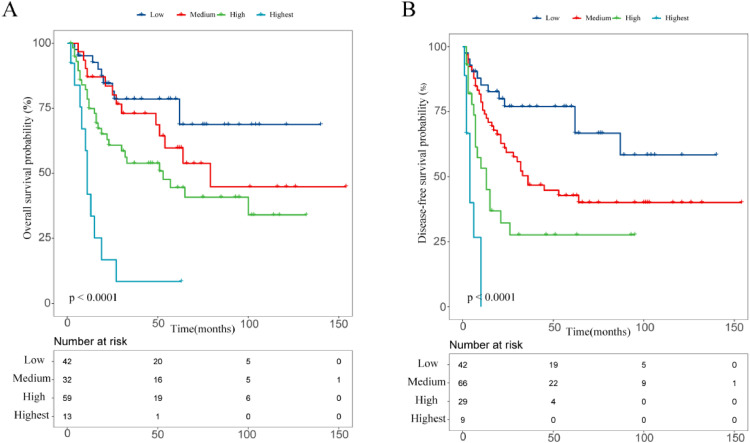
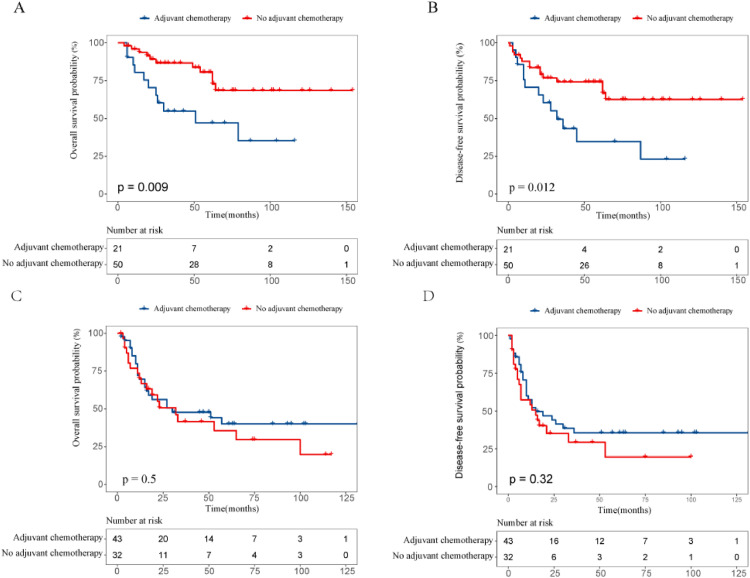
The median follow-up was 53 months. The pathological complete respond (pCR) group demonstrated better 5-year OS and DFS (78.6% and 77.0%) than the non-pCR group (44.8% and 35.2%, all P < 0.005). Multivariate analysis for the non-pCR group revealed perineural invasion (PNI) (HR:2.296, P = 0.013) and ypTNM stage (I/II vs III/IV) (HR:1.972, P = 0.046) were considered as independent unfavorable factors affecting OS, while PNI (HR:1.866, P = 0.045) and lymph vessel invasion (LVI) (HR:3.370, P < 0.001) were considered as independent adverse factors for DFS. Based on clinicopathological factors (including pCR, ypTNM stage, PNI, LVI), patients were divided into the low-risk (pCR), mediate-risk (non-pCR without PNI, LVI, stage III/IV), high-risk (non-pCR with one factor of PNI, LVI or stage III/IV (n = 45)), highest risk (non-pCR with two or more factors of PNI, LVI or stage III/IV) groups. The corresponding 5-year OS rates were 78.6%, 60.4%, 49.6%, 18.6%, respectively (P < 0.005) and 5-year DFS rates were 77.0%, 46.9%, 41.1%, 12.1%, respectively (P < 0.005). Adjuvant chemotherapy may improve survival in high or highest risk groups of patients with low prognostic nutritional index (< 49).
A novel risk stratification based on clinicopathological factors may be conducive to postoperative surveillance and guide adjuvant chemotherapy.
目前,鲜有研究报道新辅助放化疗(NCRT)及手术后食管鳞状细胞癌(ESCC)患者的风险分层。我们旨在建立一种简单的风险分层方法,以辅助术后监测及辅助治疗。
我们纳入了146例接受NCRT后行食管切除术的局部晚期ESCC患者。分析临床病理因素对总生存期(OS)和无病生存期(DFS)的影响。同时记录复发部位、时间及频率。
中位随访时间为53个月。病理完全缓解(pCR)组的5年OS和DFS表现更佳(分别为78.6%和77.0%),优于非pCR组(分别为44.8%和35.2%,P均<0.005)。对非pCR组的多因素分析显示,神经周围浸润(PNI)(HR:2.296,P = 0.013)和ypTNM分期(I/II期 vs III/IV期)(HR:1.972,P = 0.046)被视为影响OS的独立不良因素,而PNI(HR:1.866,P = 0.045)和淋巴管浸润(LVI)(HR:3.370,P < 0.001)被视为DFS的独立不良因素。基于临床病理因素(包括pCR、ypTNM分期、PNI、LVI),患者被分为低风险(pCR)、中风险(非pCR且无PNI、LVI、III/IV期)、高风险(非pCR且有PNI、LVI或III/IV期其中一个因素(n = 45))、最高风险(非pCR且有PNI、LVI或III/IV期两个或更多因素)组。相应的5年OS率分别为78.6%、60.4%、49.6%、18.6%(P < 0.005),5年DFS率分别为77.0%、46.9%、41.1%、12.1%(P < 0.005)。辅助化疗可能改善预后营养指数较低(< 49)的高风险或最高风险组患者的生存。
基于临床病理因素的新型风险分层可能有助于术后监测并指导辅助化疗。