Department of Surgery A, Galilee Medical Center, 22100, Nahariya, Israel.
Medical Corps, Israel Defense Forces, Ramat Gan, Israel.
J Med Case Rep. 2021 Feb 23;15(1):93. doi: 10.1186/s13256-020-02608-1.
Current management of choledocholithiasis entails the use of endoscopic retrograde cholangiopancreatography (ERCP) and clearance of the common bile duct. A rare complication of this procedure is the impaction of the basket by a large stone, which necessitates lithotripsy. Here we report a case of an impacted basket during ERCP, which was managed by open surgery with a duodenotomy and the manual removal of the basket.
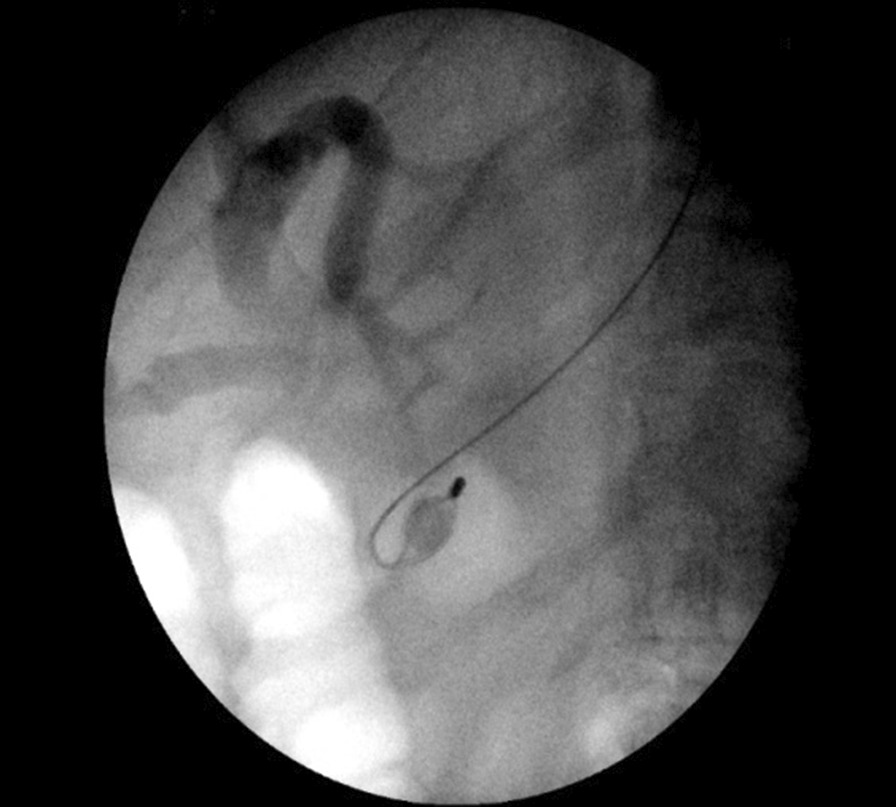
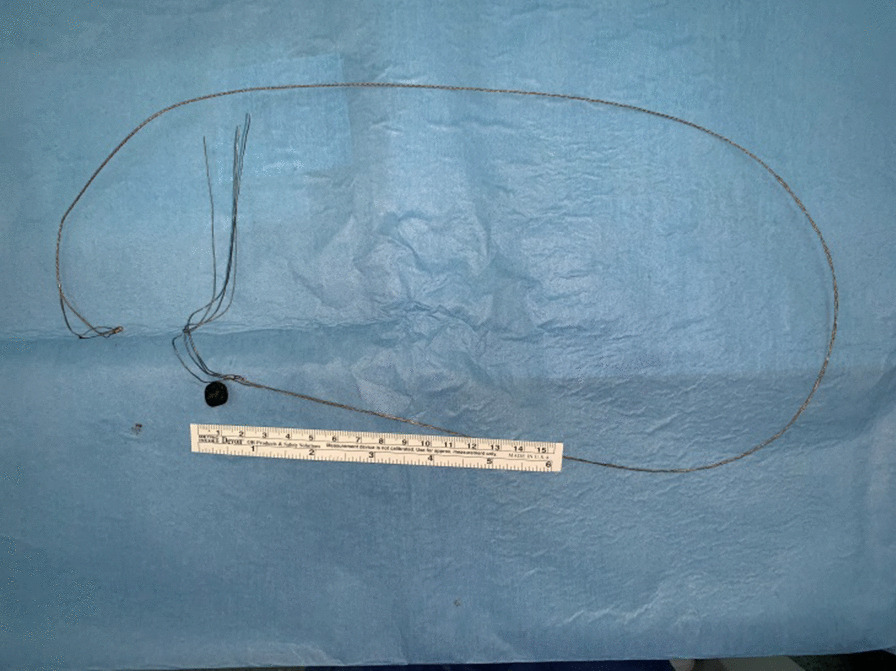
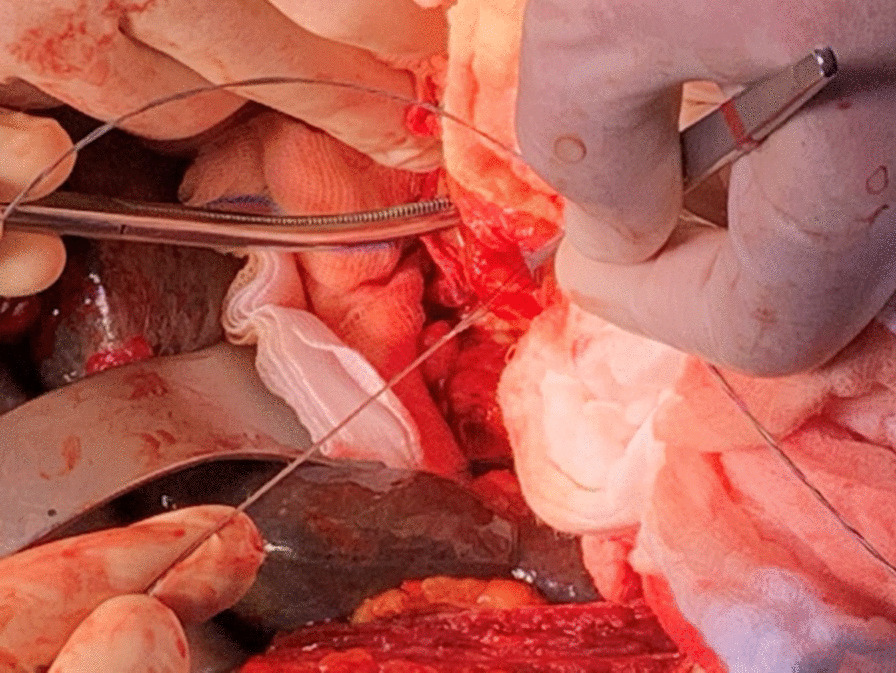
A 79-year-old Caucasian man was admitted to our department with yellowish discoloration of urine, skin and eyes. Abdominal ultrasonography showed a slightly thickened gallbladder, multiple gallbladder stones, dilated intrahepatic bile ducts and extrahepatic bile extending to 1.1 cm. A computed tomography (CT) scan demonstrated a stone in the common bile duct, which caused dilation of the biliary ducts. The patient was diagnosed with obstructive jaundice secondary to choledocholithiasis; and underwent an ERCP, a sphincterotomy and stone extraction. Four days following discharge, the patient was readmitted with jaundice, abdominal pain, vomiting and fever. He was diagnosed with ascending cholangitis and treated initially with antibiotics. A second ERCP revealed a dilated common bile duct and choledocholithiasis. Stone removal with a basket failed, as did mechanical lithotripsy. Finally, the wires of the basket were ruptured and stacked in the common bile duct together with the stone. During exploratory laparotomy, adhesiolysis, a Kocher maneuver of the duodenum and a subtotal cholecystectomy were performed. Choledochotomy did not succeed in removing the impacted wires together with the stone. Therefore, a duodenotomy and an extension of the sphincterotomy were performed, followed by high-pressure lavage of the common bile duct to remove additional small biliary stones. The choledochotomy and duodenotomy were closed by a one-layer suture, and a prophylactic gastroenterostomy was performed to prevent leakage from the common bile duct and the duodenum. The postoperative course was satisfactory.
This is the first report in the literature of removal of an impacted Dormia basket through the papilla by performing a duodenotomy and an extension of the sphincterotomy, followed by gastroenterostomy.
目前,胆总管结石的治疗需要采用内镜逆行胰胆管造影术(ERCP)并清除胆总管。该手术的一种罕见并发症是篮筐被大结石堵塞,需要碎石。在此,我们报告一例 ERCP 时篮筐嵌顿的病例,通过十二指肠切开术和手动取出篮筐进行开腹手术治疗。
一名 79 岁白人男性因尿色发黄、皮肤和眼睛发黄而入院。腹部超声显示胆囊稍增厚,多发胆囊结石,肝内胆管和肝外胆管扩张至 1.1cm。计算机断层扫描(CT)显示胆总管内有结石,导致胆管扩张。患者被诊断为胆总管结石继发的阻塞性黄疸,并进行了 ERCP、括约肌切开术和取石术。出院后 4 天,患者因黄疸、腹痛、呕吐和发热再次入院。患者被诊断为上行性胆管炎,最初给予抗生素治疗。第二次 ERCP 显示胆总管扩张和胆总管结石。篮筐取石失败,机械碎石也失败。最终,篮筐的金属丝断裂并与结石一起堆积在胆总管中。剖腹探查时进行了粘连松解、十二指肠 Kocher 操作和胆囊次全切除术。胆总管切开术未能成功取出嵌顿的金属丝和结石。因此,进行了十二指肠切开术和括约肌切开术的延长,然后对胆总管进行高压冲洗以去除额外的小胆管结石。胆总管切开术和十二指肠切开术采用单层缝合关闭,并进行预防性胃空肠吻合术以防止胆总管和十二指肠漏。术后过程满意。
这是首例通过乳头切开十二指肠和括约肌切开术延长,并进行胃空肠吻合术取出嵌顿的 Dormia 篮筐的文献报道。