Prior Lisa, Featherstone Hannah, O'Reilly David, Nugent Killian, Lim Marvin, McCaffrey John, Higgins Michaela J, Kelly Catherine M
Department of Medical Oncology, Mater Misericordiae University Hospital, Eccles St, Dublin, D07 R2WY, Ireland.
UCD (University College Dublin) School of Medicine, Belfield, Dublin 4, Ireland.
Cardiooncology. 2021 Feb 23;7(1):8. doi: 10.1186/s40959-021-00096-w.
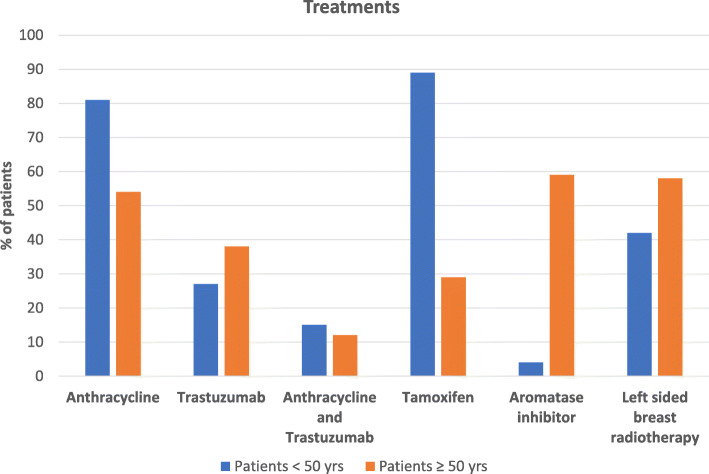
Due to advances in care, most women diagnosed with breast cancer do not die from the disease itself. Instead, cardiovascular disease (CVD) remains the most frequent cause of death. Many breast cancer patients are older and have established CVD risk factors. They are at further risk due to exposure to anthracyclines, HER2 targeted agents, endocrine therapy and radiotherapy. In this study, we compared the 10-year predicted risk of breast cancer mortality versus that of cardiovascular (CV) morbidity/mortality in breast cancer patients receiving adjuvant chemotherapy using online predictive risk calculators. Furthermore, we evaluated the predicted outcome of CV risk factor optimisation on their overall CV risk.
This was a cross sectional study. All patients with resected Stage I-III breast cancer who received adjuvant chemotherapy at our centre from September 2015 to November 2016 were identified. Data recorded included demographics, tumor characteristics, treatments and CV risk factors. To calculate predicted 10-year risk of CVD and impact of lifestyle changes, we used the JBS3 (Joint British Society) online risk calculator. To calculate the predicted 10-year risk of breast cancer mortality, we used the PREDICT calculator. Biostatistical methods included Wilcoxon signed rank test for predicted CVD risk pre and post cardiovascular risk optimization.
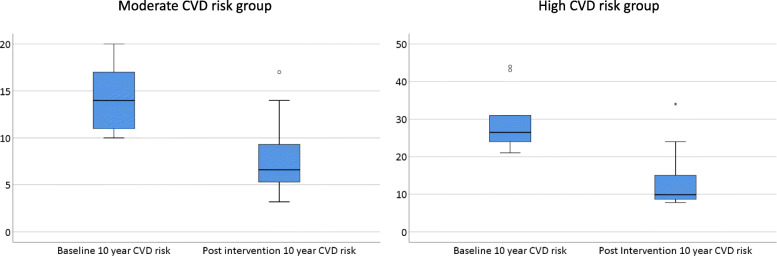
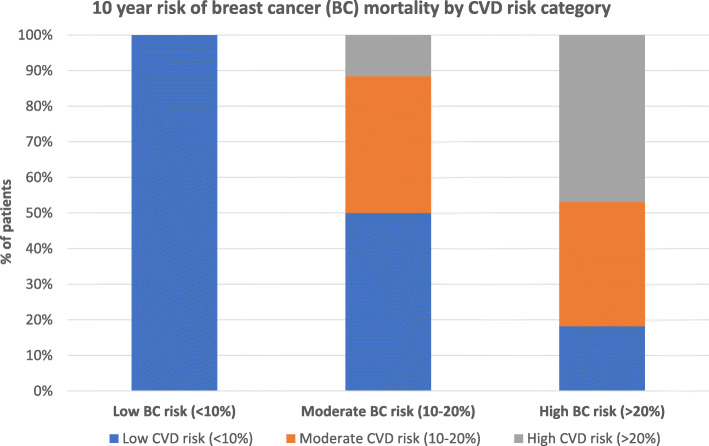
We identified 102 patients. Of this cohort, 76 patients were ≥ 50 years & 26 were < 50 years of age. The group had significant baseline cardiovascular risk factors: increased BMI (68 %, n = 70), ex-smoking (34 %, n = 35), current smoking (13 %, n = 13), hypertension (47 %, n = 47) and dyslipidemia (57 %). Of the total group, 48 % had a high (> 20 %) and 37 % had a moderate (10-20 %) 10-year predicted breast cancer mortality risk. Regarding 10-year predicted risk of CVD, 11 % and 22 % fell into the high (> 20 %) and moderate (10-20 %) risk categories, respectively. Assuming CV risk factor optimisation, there was a predicted improvement in median 10-year CV risk from 26.5 to 9.9 % (p = .005) in the high CVD risk group and from 14.0 to 6.6 % (p < .001) in the moderate CVD risk group.
Benefits predicted with a CVD risk intervention model indicates that this should be incorporated into routine breast oncology care.
由于医疗水平的进步,大多数被诊断为乳腺癌的女性并非死于该疾病本身。相反,心血管疾病(CVD)仍然是最常见的死亡原因。许多乳腺癌患者年龄较大且已存在心血管疾病风险因素。由于接触蒽环类药物、HER2靶向药物、内分泌治疗和放疗,他们面临更高的风险。在本研究中,我们使用在线预测风险计算器比较了接受辅助化疗的乳腺癌患者10年乳腺癌死亡预测风险与心血管(CV)发病/死亡风险。此外,我们评估了心血管风险因素优化对其总体心血管风险的预测结果。
这是一项横断面研究。确定了2015年9月至2016年11月在我们中心接受辅助化疗的所有I-III期乳腺癌切除患者。记录的数据包括人口统计学、肿瘤特征、治疗方法和心血管风险因素。为了计算心血管疾病的预测10年风险和生活方式改变的影响,我们使用了JBS3(英国联合协会)在线风险计算器。为了计算乳腺癌死亡的预测10年风险,我们使用了PREDICT计算器。生物统计学方法包括对心血管风险优化前后的预测心血管疾病风险进行Wilcoxon符号秩检验。
我们确定了102例患者。在这个队列中,76例患者年龄≥50岁,26例患者年龄<50岁。该组有显著的基线心血管风险因素:体重指数增加(68%,n = 70)、既往吸烟(34%,n = 35)、当前吸烟(13%,n = 13)、高血压(47%,n = 47)和血脂异常(57%)。在整个组中,48%的患者10年乳腺癌死亡预测风险高(>20%),37%的患者为中度(10-20%)。关于心血管疾病的10年预测风险,分别有11%和22%的患者属于高风险(>20%)和中度风险(10-20%)类别。假设心血管风险因素得到优化,高心血管疾病风险组的10年心血管风险中位数预计从26.5%改善至9.9%(p = 0.005),中度心血管疾病风险组从14.0%改善至6.6%(p < 0.001)。
心血管疾病风险干预模型预测的益处表明,应将其纳入常规乳腺肿瘤学护理中。