Tassiopoulos Apostolos K, Mofakham Sima, Rubano Jerry A, Labropoulos Nicos, Bannazadeh Mohsen, Drakos Panagiotis, Volteas Panagiotis, Cleri Nathaniel A, Alkadaa Leor N, Asencio Anthony A, Oganov Anthony, Hou Wei, Rutigliano Daniel N, Singer Adam J, Vosswinkel James, Talamini Mark, Mikell Charles B, Kaushansky Kenneth
Department of Surgery, Renaissance School of Medicine, Stony Brook, NY, United States.
Division of Vascular Surgery, Department of Surgery, Renaissance School of Medicine, Stony Brook, NY, United States.
Front Med (Lausanne). 2021 Feb 4;8:631335. doi: 10.3389/fmed.2021.631335. eCollection 2021.
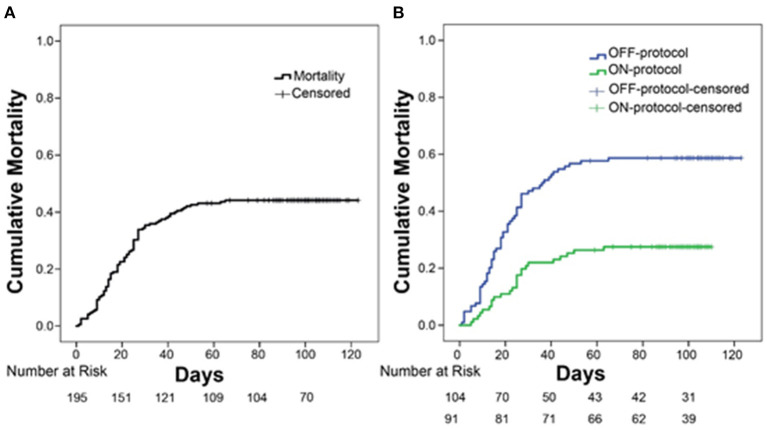
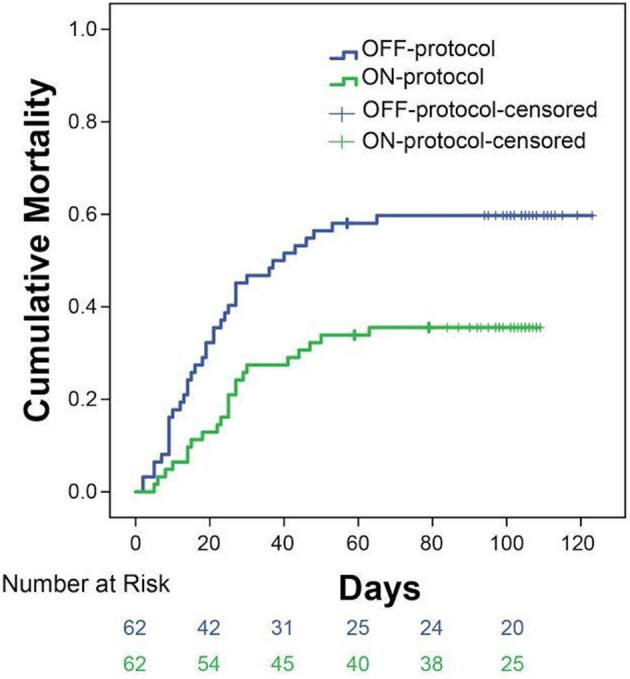
Examine the possible beneficial effects of early, D-dimer driven anticoagulation in preventing thrombotic complications and improving the overall outcomes of COVID-19 intubated patients. To address COVID-19 hypercoagulability, we developed a clinical protocol to escalate anticoagulation based on serum D-dimer levels. We retrospectively reviewed all our first 240 intubated patients with COVID-19. Of the 240, 195 were stratified into patients treated based on this protocol (ON-protocol, = 91) and the control group, patients who received standard thromboprophylaxis (OFF-protocol, = 104). All patients were admitted to the Stony Brook University Hospital intensive care units (ICUs) between February 7th, 2020 and May 17, 2020 and were otherwise treated in the same manner for all aspects of COVID-19 disease. We found that the overall mortality was significantly lower ON-protocol compared to OFF-protocol (27.47 vs. 58.66%, < 0.001). Average maximum D-dimer levels were significantly lower in the ON-protocol group (7,553 vs. 12,343 ng/mL), as was serum creatinine (2.2 vs. 2.8 mg/dL). Patients with poorly controlled D-dimer levels had higher rates of kidney dysfunction and mortality. Transfusion requirements and serious bleeding events were similar between groups. To address any possible between-group differences, we performed a propensity-matched analysis of 124 of the subjects (62 matched pairs, ON-protocol and OFF-protocol), which showed similar findings (31 vs. 57% overall mortality in the ON-protocol and OFF-protocol group, respectively). D-dimer-driven anticoagulation appears to be safe in patients with COVID-19 infection and is associated with improved survival. It has been shown that hypercoagulability in patients with severe COVID-19 infection leads to thromboembolic complications and organ dysfunction. Anticoagulation has been variably administered to these patients, but it is unknown whether routine or escalated thromboprophylaxis provides a survival benefit. Our data shows that escalated D-dimer driven anticoagulation is associated with improved organ function and overall survival in intubated COVID-19 ICU patients at our institution. Importantly, we found that timely escalation of this anticoagulation is critical in preventing organ dysfunction and mortality in patients with severe COVID-19 infection.
研究早期D - 二聚体驱动的抗凝治疗在预防血栓形成并发症和改善COVID - 19插管患者总体预后方面可能的有益效果。为应对COVID - 19的高凝状态,我们制定了一项基于血清D - 二聚体水平逐步加强抗凝治疗的临床方案。我们回顾性分析了我院首批240例COVID - 19插管患者。在这240例患者中,195例被分层为根据该方案接受治疗的患者(方案组,n = 91)和对照组,即接受标准血栓预防措施的患者(非方案组,n = 104)。所有患者均于2020年2月7日至2020年5月17日入住石溪大学医院重症监护病房(ICU),并且在COVID - 19疾病的各个方面均接受相同方式的治疗。我们发现,与非方案组相比,方案组的总体死亡率显著更低(27.47%对58.66%,P < 0.001)。方案组的平均最大D - 二聚体水平显著更低(7553对12343 ng/mL),血清肌酐水平也是如此(2.2对2.8 mg/dL)。D - 二聚体水平控制不佳的患者肾功能不全和死亡率更高。两组之间的输血需求和严重出血事件相似。为解决任何可能的组间差异,我们对124名受试者(62对匹配,方案组和非方案组)进行了倾向匹配分析,结果显示了相似的结果(方案组和非方案组的总体死亡率分别为31%和57%)。D - 二聚体驱动的抗凝治疗在COVID - 19感染患者中似乎是安全的,并且与生存率提高相关。已表明,重症COVID - 19感染患者的高凝状态会导致血栓栓塞并发症和器官功能障碍。已对这些患者采用了不同的抗凝治疗,但常规或强化血栓预防是否能带来生存获益尚不清楚。我们的数据表明,在我们机构中,强化的D - 二聚体驱动的抗凝治疗与COVID - 19插管ICU患者的器官功能改善和总体生存改善相关。重要的是,我们发现及时加强这种抗凝治疗对于预防重症COVID - 19感染患者的器官功能障碍和死亡至关重要。