Helms Julie, Severac François, Merdji Hamid, Schenck Maleka, Clere-Jehl Raphaël, Baldacini Mathieu, Ohana Mickaël, Grunebaum Lélia, Castelain Vincent, Anglés-Cano Eduardo, Sattler Laurent, Meziani Ferhat
Service de Médecine Intensive Réanimation, Nouvel Hôpital Civil, Hôpitaux Universitaires de Strasbourg, 1, Place de l'Hôpital, 67091, Strasbourg Cedex, France.
ImmunoRhumatologie Moléculaire, INSERM UMR_S1109, LabEx TRANSPLANTEX, Centre de Recherche d'Immunologie et d'Hématologie, Faculté de Médecine, Fédération Hospitalo-Universitaire (FHU) OMICARE, Fédération de Médecine Translationnelle de Strasbourg (FMTS), Université de Strasbourg (UNISTRA), Strasbourg, France.
Ann Intensive Care. 2021 Jan 25;11(1):14. doi: 10.1186/s13613-021-00809-5.
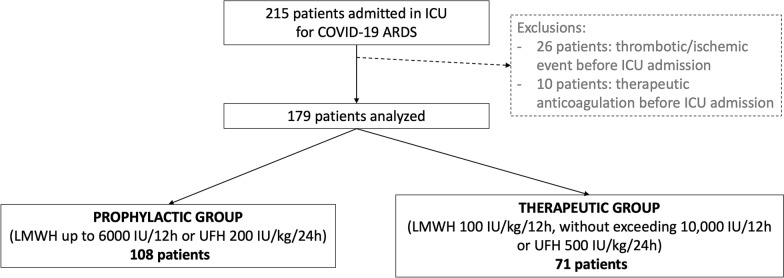
Thromboprophylaxis of COVID-19 patients is a highly debated issue. We aimed to compare the occurrence of thrombotic/ischemic events in COVID-19 patients with acute respiratory distress syndrome (ARDS) treated with either prophylactic or therapeutic dosage of heparin. All patients referred for COVID-19 ARDS in two intensive care units (ICUs) from two centers of a French tertiary hospital were included in our cohort study. Patients were compared according to their anticoagulant treatment to evaluate the risk/benefit of prophylactic anticoagulation versus therapeutic anticoagulation. Medical history, symptoms, biological data and imaging were prospectively collected.
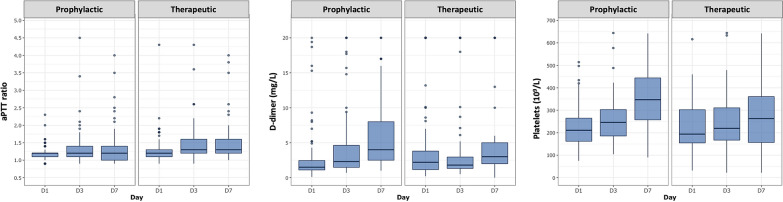
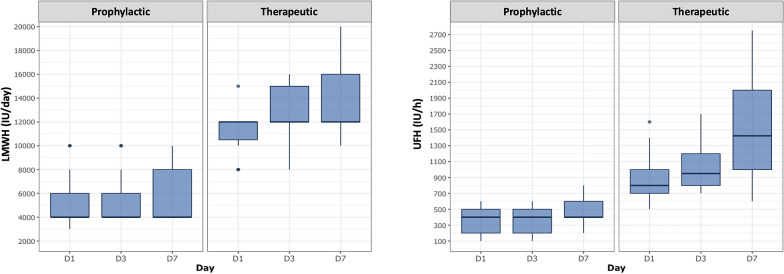
One hundred and seventy-nine patients (73% men) were analyzed: 108 in prophylactic group and 71 in therapeutic group. Median age and SAPS II were 62 [IQR 51; 70] years and 47 [IQR 37; 63] points. ICU mortality rate was 17.3%. Fifty-seven patients developed clinically relevant thrombotic complications during their ICU stay, less frequently in therapeutic group (adjusted OR 0.38 [0.14-0.94], p = 0.04). The occurrences of pulmonary embolism (PE), deep vein thrombosis (DVT) and ischemic stroke were significantly lower in the therapeutic group (respective adjusted OR for PE: 0.19 [0.03-0.81]; DVT: 0.13 [0.01-0.89], stroke: 0.06 [0-0.68], all p < 0.05). The occurrence of bleeding complications was not significantly different between groups, neither were ICU length of stay or mortality rate. D-dimer levels were significantly lower during ICU stay, and aPTT ratio was more prolonged in the therapeutic group (p < 0.05).
Increasing the anticoagulation of severe COVID-19 patients to a therapeutic level might decrease thrombotic complications without increasing their bleeding risk.
新型冠状病毒肺炎(COVID-19)患者的血栓预防是一个备受争议的问题。我们旨在比较接受预防性或治疗性剂量肝素治疗的急性呼吸窘迫综合征(ARDS)COVID-19患者发生血栓形成/缺血性事件的情况。我们的队列研究纳入了法国一家三级医院两个中心的两个重症监护病房(ICU)中所有因COVID-19 ARDS转诊的患者。根据抗凝治疗情况对患者进行比较,以评估预防性抗凝与治疗性抗凝的风险/益处。前瞻性收集病史、症状、生物学数据和影像学资料。
共分析了179例患者(73%为男性):预防性治疗组108例,治疗性治疗组71例。中位年龄和简化急性生理学评分(SAPS)II分别为62[四分位间距(IQR)51;70]岁和47[IQR 37;63]分。ICU死亡率为17.3%。57例患者在ICU住院期间发生了临床相关的血栓并发症,治疗性治疗组的发生率较低(校正比值比0.38[0.14 - 0.94],p = 0.04)。治疗性治疗组的肺栓塞(PE)、深静脉血栓形成(DVT)和缺血性卒中的发生率显著较低(PE的校正比值比分别为:0.19[0.03 - 0.81];DVT:0.13[0.01 - 0.89],卒中:0.06[0 - 0.68],均p < 0.05)。两组出血并发症的发生率无显著差异,ICU住院时间或死亡率也无显著差异。ICU住院期间D-二聚体水平显著降低,治疗性治疗组活化部分凝血活酶时间(aPTT)比值延长更明显(p < 0.05)。
将重症COVID-19患者的抗凝水平提高到治疗水平可能会降低血栓并发症,而不会增加出血风险。