Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical CenterHarvard Medical School Boston MA.
Department of Anesthesia, Critical Care and Pain Medicine Massachusetts General HospitalHarvard Medical School Boston MA.
J Am Heart Assoc. 2021 Feb;10(5):e018952. doi: 10.1161/JAHA.120.018952. Epub 2021 Feb 26.
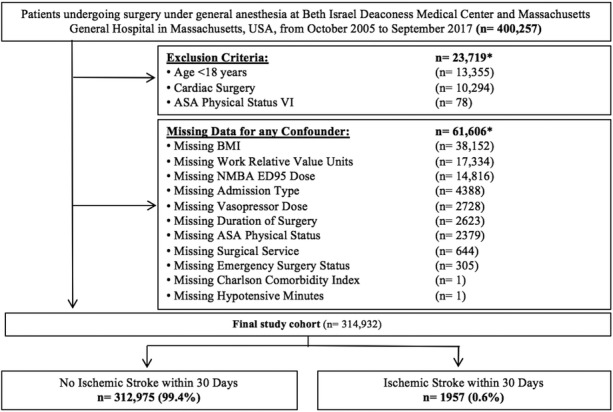
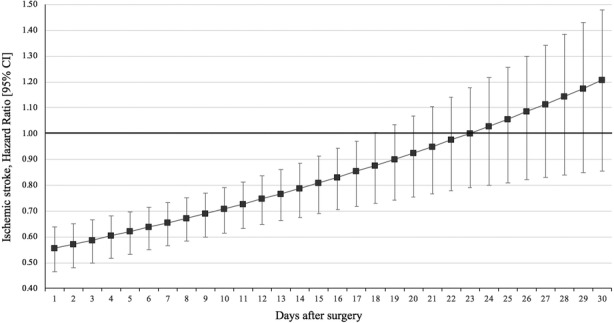
Background Preclinical studies suggest that volatile anesthetics decrease infarct volume and improve the outcome of ischemic stroke. This study aims to determine their effect during noncardiac surgery on postoperative ischemic stroke incidence. Methods and Results This was a retrospective cohort study of surgical patients undergoing general anesthesia at 2 tertiary care centers in Boston, MA, between October 2005 and September 2017. Exclusion criteria comprised brain death, age <18 years, cardiac surgery, and missing covariate data. The exposure was defined as median age-adjusted minimum alveolar concentration of all intraoperative measurements of desflurane, sevoflurane, and isoflurane. The primary outcome was postoperative ischemic stroke within 30 days. Among 314 932 patients, 1957 (0.6%) experienced the primary outcome. Higher doses of volatile anesthetics had a protective effect on postoperative ischemic stroke incidence (adjusted odds ratio per 1 minimum alveolar concentration increase 0.49, 95% CI, 0.40-0.59, <0.001). In Cox proportional hazards regression, the effect was observed for 17 postoperative days (postoperative day 1: hazard ratio (HR), 0.56; 95% CI, 0.48-0.65; versus day 17: HR, 0.85; 95% CI, 0.74-0.99). Volatile anesthetics were also associated with lower stroke severity: Every 1-unit increase in minimum alveolar concentration was associated with a 0.006-unit decrease in the National Institutes of Health Stroke Scale (95% CI, -0.01 to -0.002, =0.002). The effects were robust throughout various sensitivity analyses including adjustment for anesthesia providers as random effect. Conclusions Among patients undergoing noncardiac surgery, volatile anesthetics showed a dose-dependent protective effect on the incidence and severity of early postoperative ischemic stroke.
临床前研究表明,挥发性麻醉剂可减少梗死体积并改善缺血性脑卒中的预后。本研究旨在确定其在非心脏手术期间对术后缺血性脑卒中发生率的影响。
这是一项回顾性队列研究,纳入了 2005 年 10 月至 2017 年 9 月在马萨诸塞州波士顿的 2 家三级保健中心接受全身麻醉的手术患者。排除标准包括脑死亡、年龄<18 岁、心脏手术以及缺失协变量数据。暴露定义为所有术中测量的地氟烷、七氟烷和异氟烷的中位数年龄调整最低肺泡浓度。主要结局为术后 30 天内发生缺血性脑卒中。在 314932 例患者中,1957 例(0.6%)发生了主要结局。挥发性麻醉剂剂量越高,对术后缺血性脑卒中发生率具有保护作用(每增加 1 个最低肺泡浓度,调整后的优势比为 0.49,95%CI:0.40-0.59,<0.001)。在 Cox 比例风险回归中,该效应持续了 17 个术后日(术后第 1 天:风险比(HR)为 0.56;95%CI:0.48-0.65;第 17 天:HR 为 0.85;95%CI:0.74-0.99)。挥发性麻醉剂也与较低的脑卒中严重程度相关:最低肺泡浓度每增加 1 个单位,NIHSS 评分降低 0.006 个单位(95%CI:-0.01 至 -0.002,=0.002)。在包括将麻醉提供者作为随机效应进行调整的各种敏感性分析中,这些效果都是稳健的。
在接受非心脏手术的患者中,挥发性麻醉剂对术后早期缺血性脑卒中的发生率和严重程度呈剂量依赖性保护作用。