Department of Obstetrics and Gynecology, Seoul National University College of Medicine, Seoul, Korea.
Seoul National University Hospital Biomedical Research Institute, Seoul, Korea.
Yonsei Med J. 2021 Mar;62(3):231-239. doi: 10.3349/ymj.2021.62.3.231.
To determine whether the prognostic impact of lymph node ratio (LNR), defined as the ratio between the number of positive lymph nodes and removed lymph nodes, differs between open and minimally invasive surgical approaches for radical hysterectomy (RH) in node-positive, early-stage cervical cancer.
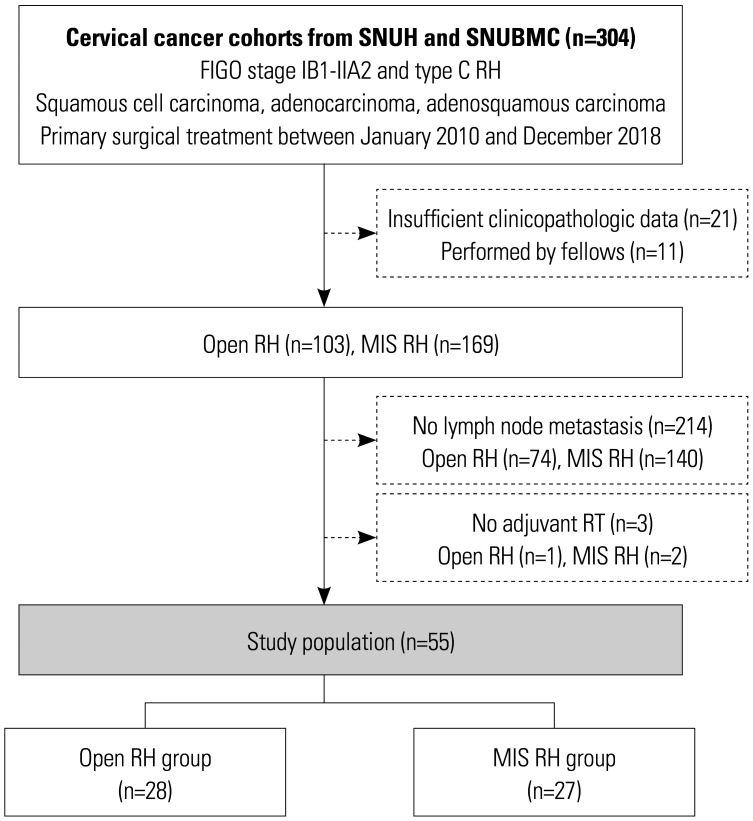
We retrospectively identified 2009 International Federation of Gynecology and Obstetrics stage IB1-IIA2 patients who underwent primary type C RH between 2010 and 2018. Among them, only those with pathologically proven lymph node metastases who received adjuvant radiation therapy were included. The prognostic significance of LNR was investigated according to open surgery and minimally invasive surgery (MIS).
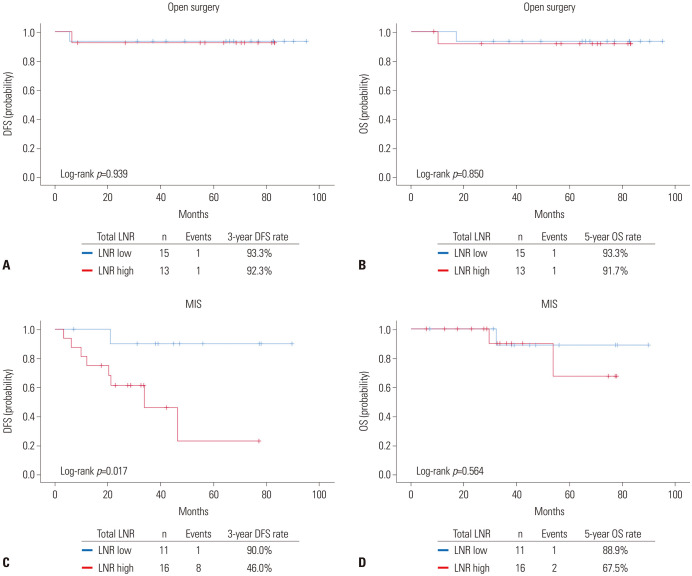
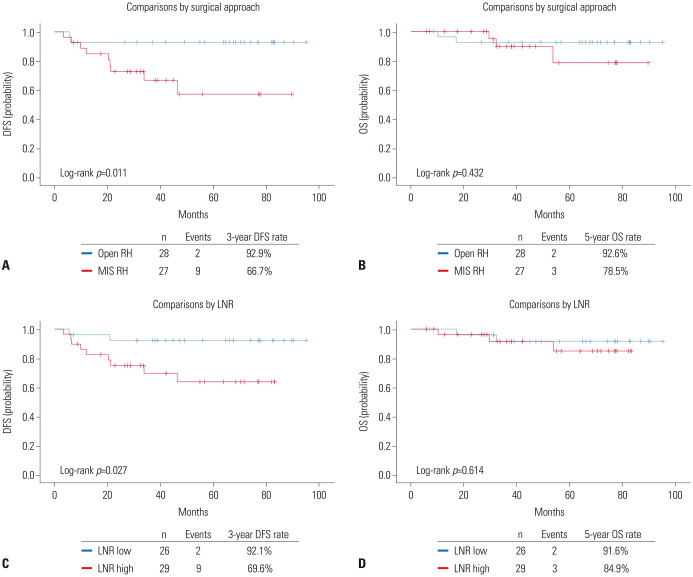
In total, 55 patients were included. The median LNR (%) was 9.524 (range, 2.083-62.500). Based on receiver operating characteristic curve analysis, the cut-off value for LNR (%) was determined as 8.831. Overall, patients with high LNR (≥8.831%; n=29) showed worse disease-free survival (DFS) than those with low LNR (<8.831%, n=26) (=0.027), whereas no difference in overall survival was observed. Multivariate analyses adjusting for clinicopathologic factors revealed that DFS was adversely affected by both MIS [adjusted hazard ratio (HR), 8.132; =0.038] and high LNR (adjusted HR, 10.837; =0.045). In a subgroup of open surgery cases, LNR was not associated with disease recurrence. However, in a subgroup of MIS cases, high LNR was identified as an independent poor prognostic factor for DFS (adjusted HR, 14.578; =0.034).
In patients with node-positive, early-stage cervical cancer, high LNR was associated with a significantly higher disease recurrence rate. This relationship was further consolidated among patients who received MIS RH.
确定在淋巴结阳性、早期宫颈癌中,以阳性淋巴结数量与切除淋巴结数量之比定义的淋巴结比率(LNR)对根治性子宫切除术(RH)的开放性和微创性手术方法的预后影响是否不同。
我们回顾性地确定了 2010 年至 2018 年间接受原发性 C 型 RH 的 2009 例国际妇产科联合会(FIGO)分期 IB1-IIA2 期患者。其中,仅纳入接受辅助放疗且有病理证实淋巴结转移的患者。根据开放性手术和微创手术(MIS)研究了 LNR 的预后意义。
共纳入 55 例患者。中位 LNR(%)为 9.524(范围,2.083-62.500)。基于接收者操作特征曲线分析,确定 LNR(%)的截断值为 8.831。总体而言,LNR 较高(≥8.831%;n=29)的患者无病生存(DFS)较 LNR 较低(<8.831%,n=26)的患者差(=0.027),但总生存无差异。调整临床病理因素的多变量分析显示,DFS 受 MIS(调整后的危险比[HR],8.132;=0.038)和高 LNR(调整后的 HR,10.837;=0.045)的不利影响。在开放性手术病例亚组中,LNR 与疾病复发无关。然而,在 MIS 病例亚组中,高 LNR 是 DFS 的独立不良预后因素(调整后的 HR,14.578;=0.034)。
在淋巴结阳性、早期宫颈癌患者中,高 LNR 与疾病复发率显著升高相关。在接受 MIS RH 的患者中,这种关系进一步得到了巩固。