Division of Internal Medicine, University Medical Center Utrecht, University of Utrecht, Utrecht, the Netherlands.
ArboUnie Occupational Health Service, Utrecht, the Netherlands.
PLoS One. 2021 Feb 26;16(2):e0246658. doi: 10.1371/journal.pone.0246658. eCollection 2021.
Calculating a modelled workload based on objective measures. Exploring the relation between this modelled workload and workload as perceived by nurses, including the effects of specific job demands, job resources and personal resources on the relation.
Academic hospital in the Netherlands. Six surgical wards, capacity 15-30 beds. Data collected over 15 consecutive day shifts.
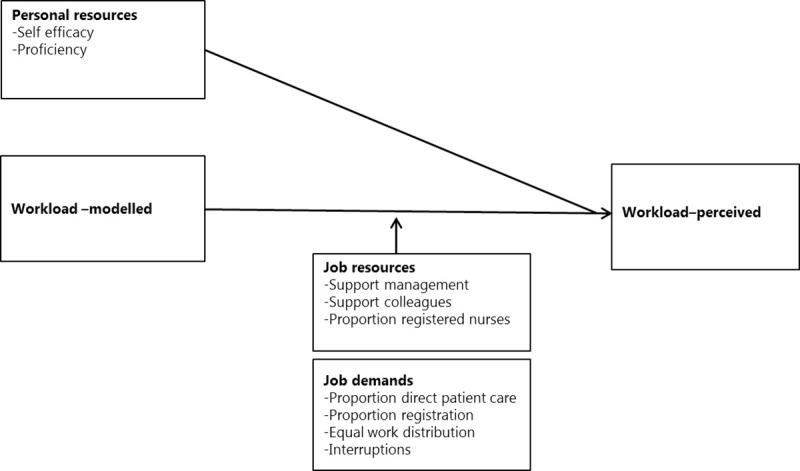
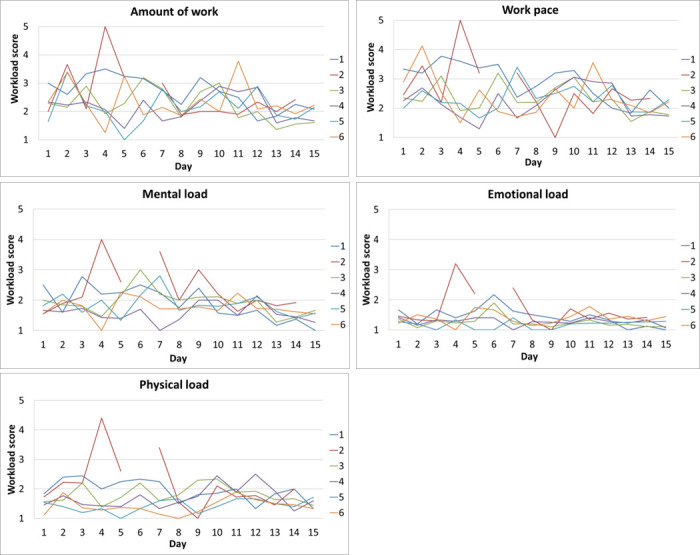
Modelled workload is calculated as a ratio of required care time, based on patient characteristics, baseline care time and time for non-patient related activities, and allocated care time, based on the amount of available nurses. Both required and allocated care time are corrected for nurse proficiency. Five dimensions of perceived workload were determined by questionnaires. Both the modelled and the perceived workloads were measured on a daily basis. Linear mixed effects models study the longitudinal relation between this modelled and workload as perceived by nurses and the effects of personal resources, job resources and job demands. ANOVA and post-hoc tests were used to identify differences in modelled workload between wards.
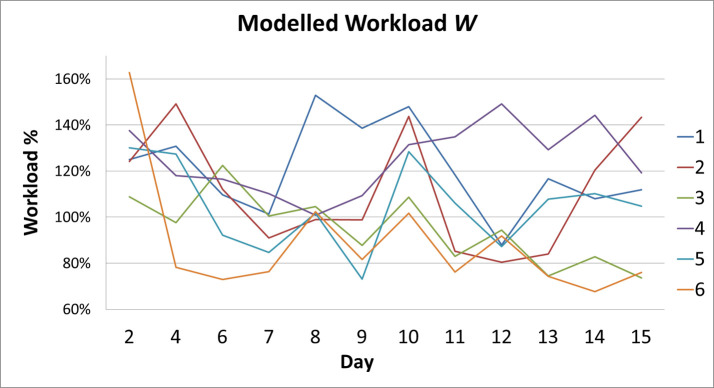
Modelled workload varies roughly between 70 and 170%. Significant differences in modelled workload between wards were found but confidence intervals were wide. Modelled workload is positively associated with all five perceived workload measures (work pace, amount of work, mental load, emotional load, physical load). In addition to modelled workload, the job resource support of colleagues and job demands time spent on direct patient care and time spent on registration had the biggest significant effects on perceived workload.
The modelled workload does not exactly predict perceived workload, however there is a correlation between the two. The modelled workload can be used to detect differences in workload between wards, which may be useful in distributing workload more evenly in order prevent issues of over- and understaffing and organizational justice. Extra effort to promote team work is likely to have a positive effect on perceived workload. Nurse management can stimulate team cohesion, especially when workload is high. Registered nurses perceive a higher workload than other nurses. When the proportion of direct patient care in a workday is higher, the perceived workload is also higher. Further research is recommended. The findings of this research can help nursing management in allocating resources and directing their attention to the most relevant factors for balancing workload.
基于客观测量指标计算模拟工作量。探索该模拟工作量与护士感知工作量之间的关系,包括特定工作要求、工作资源和个人资源对这种关系的影响。
荷兰某学术医院。六个外科病房,床位 15-30 张。在 15 个连续的白班期间收集数据。
模拟工作量是根据患者特征、基线护理时间和非患者相关活动时间以及基于可用护士数量的分配护理时间计算出来的所需护理时间的比率。所需和分配的护理时间都经过护士熟练程度的校正。通过问卷确定了五个感知工作量维度。模拟和感知工作量都是每天进行测量。线性混合效应模型研究了模拟和护士感知工作量之间的纵向关系,以及个人资源、工作资源和工作要求的影响。方差分析和事后检验用于确定病房之间的模拟工作量差异。
模拟工作量大致在 70%到 170%之间变化。发现病房之间的模拟工作量存在显著差异,但置信区间较宽。模拟工作量与五个感知工作量测量值(工作节奏、工作量、心理负荷、情绪负荷、体力负荷)均呈正相关。除了模拟工作量外,同事的工作资源支持以及直接病人护理时间和登记时间等工作要求对感知工作量的影响最大。
模拟工作量并不能准确预测感知工作量,但两者之间存在相关性。模拟工作量可用于检测病房之间的工作量差异,这对于更均匀地分配工作量以防止人员超编和欠编以及组织公平问题可能是有用的。促进团队合作的额外努力可能会对感知工作量产生积极影响。注册护士比其他护士感知到的工作量更高。当工作日内直接病人护理的比例较高时,感知工作量也较高。建议进一步研究。这项研究的结果可以帮助护理管理部门分配资源,并将注意力集中在平衡工作量的最相关因素上。