Kinshasa School of Public Health, Faculty of Medicine, University of Kinshasa, Kinshasa, Democratic Republic of Congo.
Pôle D'Épidémiologie et Biostatistique, Institut de Recherche Expérimentale et Clinique (IREC), Université Catholique de Louvain (UCLouvain), Clos Chapelle-aux-champs, 30 bte B1.30.13, 1200, Brussels, Belgium.
BMC Womens Health. 2021 Feb 26;21(1):82. doi: 10.1186/s12905-021-01234-3.
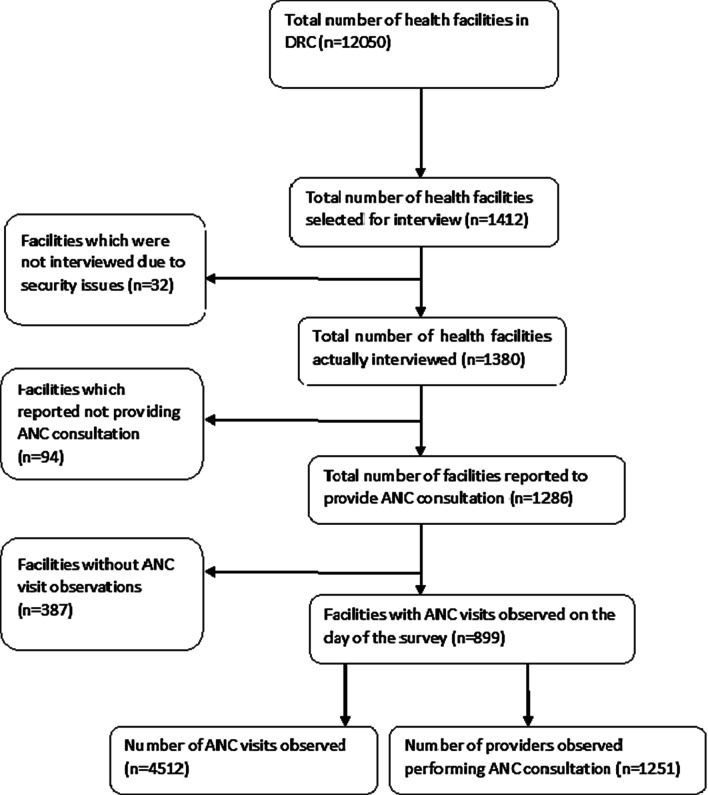
Poor awareness of obstetric danger signs is a major contributing factor to delays in seeking obstetric care and hence to high maternal mortality and morbidity worldwide. We conducted the current study to assess the level of agreement on receipt of counseling on obstetric danger signs between direct observations of antenatal care (ANC) consultation and women's recall in the exit interview. We also identified factors associated with pregnant women's awareness of obstetric danger signs during pregnancy in the Democratic Republic of Congo (DRC) METHODS: We used data from the 2017-2018 DRC Service Provision Assessment survey. Agreement between the observation and woman's recall was measured using Cohen's kappa statistic and percent agreement. Multivariable Zero-Inflated Poisson (ZIP) regression was used to identify factors associated with the number of danger signs during pregnancy the woman knew.
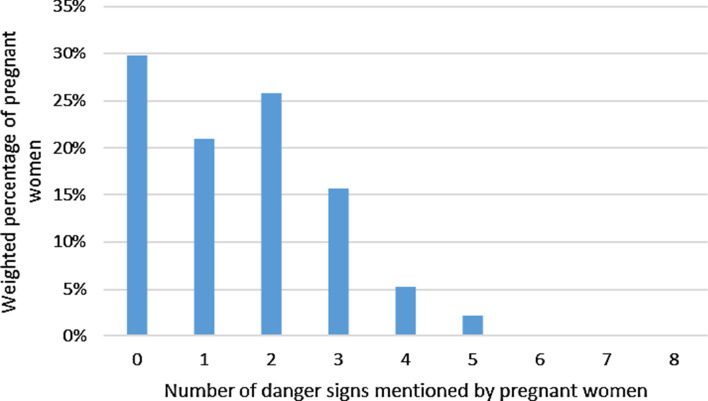
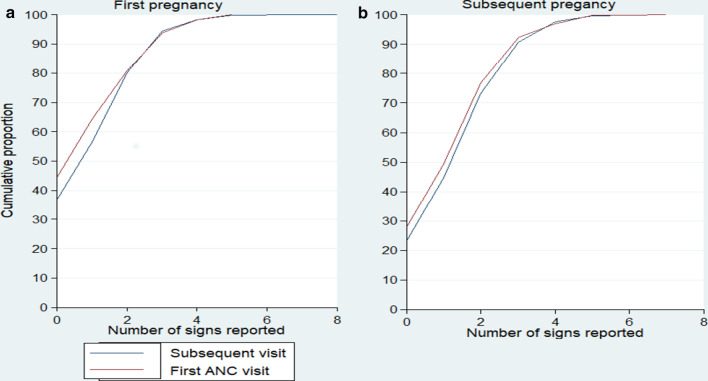
On average, women were aware of 1.5 ± 1.34 danger signs in pregnancy (range: 0 to 8). Agreement between observation and woman's recall was 70.7%, with a positive agreement of 16.9% at the country level but ranging from 2.1% in Bandundu to 39.7% in Sud Kivu. Using multivariable ZIP analysis, the number of obstetric danger signs the women mentioned was significantly higher in multigravida women (Adj.IRR = 1.38; 95% CI: 1.23-1.55), in women attending a private facility (Adj.IRR = 1.15; 95% CI: 1.01-1.31), in women attending a subsequent ANC visit (Adj.IRR = 1.11; 95% CI: 1.01-1.21), and in women counseled on danger signs during the ANC visit (Adj.IRR = 1.19; 95% CI: 1.05-1.35). There was a regional variation in the awareness of danger signs, with the least mentioned signs in the middle and the most in the eastern provinces.
Our findings indicated poor agreement between directly observed counseling and women's reports that counseling on obstetric danger signs occurred during the current ANC visit. We found that province of residence, provision of counseling on obstetric danger signs, facility ownership, gravidity and the number of ANC visits were predictors of the awareness of obstetric danger signs among pregnant women. These factors should be considered when developing strategies aim at improving women's awareness about obstetric danger signs in the DRC.
对产科危险信号的认识不足是导致全球寻求产科护理延迟的主要因素,从而导致孕产妇死亡率和发病率居高不下。我们进行了当前的研究,以评估直接观察产前保健 (ANC) 咨询与妇女在出口访谈中回忆之间关于产科危险信号接受咨询的一致性。我们还确定了与刚果民主共和国 (DRC) 怀孕期间孕妇对产科危险信号的认识相关的因素。
我们使用了 2017-2018 年刚果民主共和国服务提供评估调查的数据。使用 Cohen's kappa 统计量和百分比一致性来衡量观察值和妇女回忆之间的一致性。使用零膨胀泊松 (ZIP) 回归模型来确定与怀孕期间妇女知晓的危险信号数量相关的因素。
平均而言,妇女在怀孕期间知晓 1.5±1.34 个危险信号(范围:0 至 8)。观察值和妇女回忆之间的一致性为 70.7%,在国家一级的阳性一致性为 16.9%,但范围从班顿杜的 2.1%到南基伍的 39.7%。使用多变量 ZIP 分析,多产妇妇女(调整后的发病率比 [IRR] = 1.38;95%置信区间:1.23-1.55)、在私立机构就诊的妇女(调整后的 IRR = 1.15;95%置信区间:1.01-1.31)、在随后的 ANC 就诊的妇女(调整后的 IRR = 1.11;95%置信区间:1.01-1.21)和在 ANC 就诊时接受危险信号咨询的妇女(调整后的 IRR = 1.19;95%置信区间:1.05-1.35)提到的产科危险信号数量明显更高。在危险信号的认识方面存在区域差异,中部地区提到的信号最少,东部省份提到的信号最多。
我们的研究结果表明,直接观察到的咨询与妇女报告的当前 ANC 就诊期间进行产科危险信号咨询之间的一致性较差。我们发现,居住地、产科危险信号咨询的提供、医疗机构的所有权、产妇的生育次数和 ANC 就诊次数是孕妇对产科危险信号认识的预测因素。在制定旨在提高刚果民主共和国妇女对产科危险信号认识的战略时,应考虑这些因素。