Bonnet Nicolas, Martin Olivier, Boubaya Marouane, Levy Vincent, Ebstein Nathan, Karoubi Philippe, Tandjaoui-Lambiotte Yacine, Van Der Meersch Guillaume, Oziel Johanna, Soulie Marie, Ghalayini Mohamed, Winchenne Anais, Zahar Jean Ralph, Ahmed Passem, Gaudry Stéphane, Cohen Yves
Intensive Care Unit, CHU Avicenne, Groupe Hospitalier Paris Seine Saint-Denis, AP-HP, 125 rue de Stalingrad, 93000, Bobigny, France.
UFR SMBH, Université Sorbonne Paris Nord, Bobigny, France.
Ann Intensive Care. 2021 Feb 27;11(1):37. doi: 10.1186/s13613-021-00825-5.
The efficacy of high flow nasal canula oxygen therapy (HFNO) to prevent invasive mechanical ventilation (IMV) is not well established in severe coronavirus disease 2019 (COVID-19). The aim of this study was to compare the risk of IMV between two strategies of oxygenation (conventional oxygenation and HFNO) in critically ill COVID 19 patients.
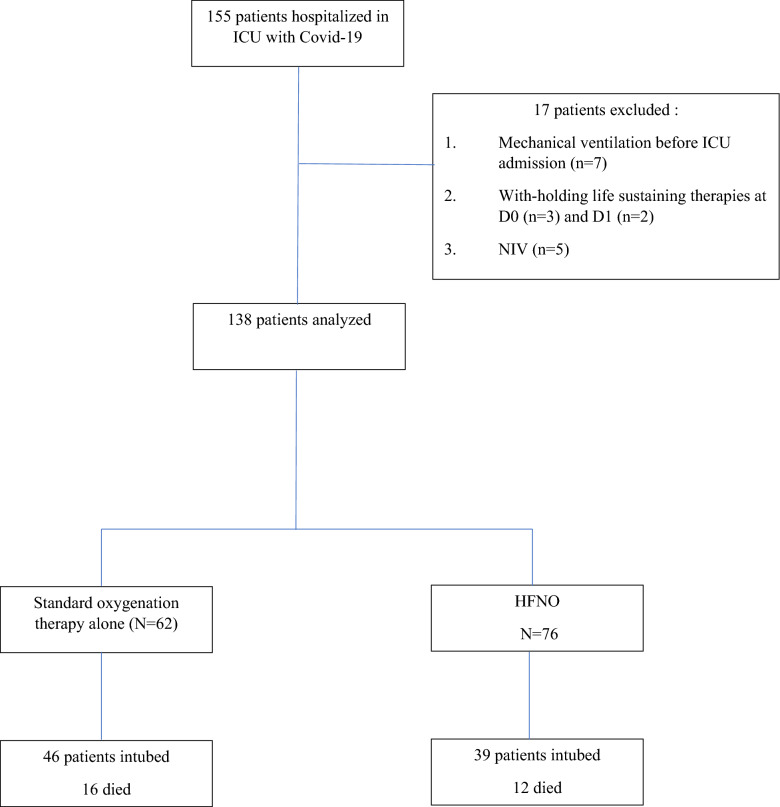
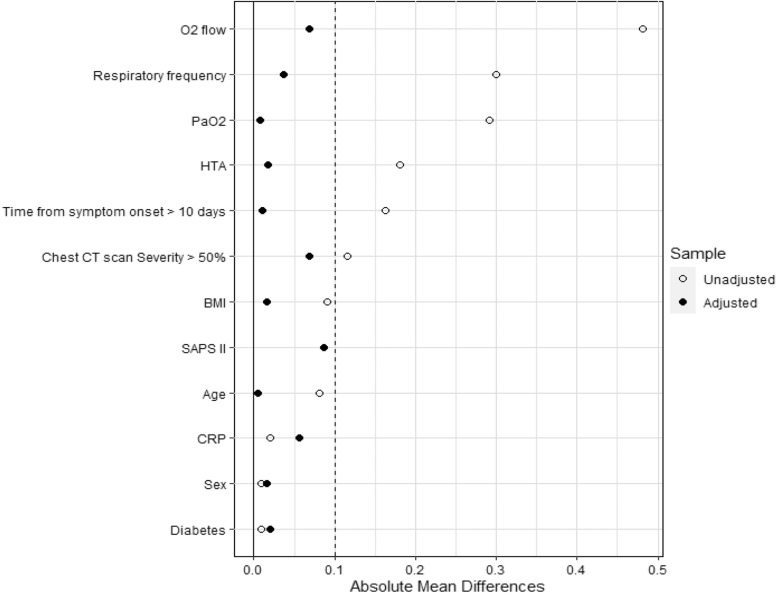
This was a bicenter retrospective study which took place in two intensive care units (ICU) of tertiary hospitals in the Paris region from March 11, to May 3, 2020. We enrolled consecutive patients hospitalized for COVID-19 and acute respiratory failure (ARF) who did not receive IMV at ICU admission. The primary outcome was the rate of IMV after ICU admission. Secondary outcomes were death at day 28 and day 60, length of ICU stay and ventilator-free days at day 28. Data from the HFNO group were compared with those from the standard oxygen therapy (SOT) group using weighted propensity score.
Among 138 patients who met the inclusion criteria, 62 (45%) were treated with SOT alone, and 76 (55%) with HFNO. In HFNO group, 39/76 (51%) patients received IMV and 46/62 (74%) in SOT group (OR 0.37 [95% CI, 0.18-0.76] p = 0.007). After weighted propensity score, HFNO was still associated with a lower rate of IMV (OR 0.31 [95% CI, 0.14-0.66] p = 0.002). Length of ICU stay and mortality at day 28 and day 60 did not significantly differ between HFNO and SOT groups after weighted propensity score. Ventilator-free days at days 28 was higher in HNFO group (21 days vs 10 days, p = 0.005). In the HFNO group, predictive factors associated with IMV were SAPS2 score (OR 1.13 [95%CI, 1.06-1.20] p = 0.0002) and ROX index > 4.88 (OR 0.23 [95%CI, 0.008-0.64] p = 0.006).
High flow nasal canula oxygen for ARF due to COVID-19 is associated with a lower rate of invasive mechanical ventilation.
在重症2019冠状病毒病(COVID-19)中,高流量鼻导管吸氧疗法(HFNO)预防有创机械通气(IMV)的疗效尚未明确。本研究旨在比较重症COVID-19患者两种氧疗策略(传统氧疗和HFNO)下IMV的风险。
这是一项双中心回顾性研究,于2020年3月11日至5月3日在巴黎地区三级医院的两个重症监护病房(ICU)进行。我们纳入了因COVID-19和急性呼吸衰竭(ARF)住院、在ICU入院时未接受IMV的连续患者。主要结局是ICU入院后IMV的发生率。次要结局是第28天和第60天的死亡率、ICU住院时间以及第28天无呼吸机天数。使用加权倾向评分将HFNO组的数据与标准氧疗(SOT)组的数据进行比较。
在138例符合纳入标准的患者中,62例(45%)仅接受SOT治疗,76例(55%)接受HFNO治疗。在HFNO组中,39/76(51%)的患者接受了IMV,SOT组为46/62(74%)(比值比0.37 [95%置信区间,0.18 - 0.76],p = 0.007)。经过加权倾向评分后,HFNO与较低的IMV发生率仍相关(比值比0.31 [95%置信区间,0.14 - 0.66],p = 0.002)。加权倾向评分后,HFNO组和SOT组在ICU住院时间以及第28天和第60天的死亡率方面无显著差异。HNFO组第28天的无呼吸机天数更高(21天对10天,p = 0.005)。在HFNO组中,与IMV相关的预测因素是序贯器官衰竭评估(SOFA)评分(比值比1.13 [95%置信区间,1.06 - 1.20],p = 0.0002)和氧合指数> 4.88(比值比0.23 [95%置信区间,0.008 - 0.64],p = 0.006)。
因COVID-19导致急性呼吸衰竭时,高流量鼻导管吸氧与较低的有创机械通气发生率相关。