Mali International Center for Excellence in Research (ICER), University of Sciences, Techniques, and Technologies of Bamako (USTTB), Bamako, Mali.
Interdisciplinary School of Health Sciences | Faculty of Health Sciences, University of Ottawa, 75, av. Laurier Est, Ottawa ON K1N 6N5, Canada.
BMC Public Health. 2021 Feb 28;21(1):421. doi: 10.1186/s12889-021-10481-w.
In Mali, nomadic populations are spread over one third of the territory. Their lifestyle, characterized by constant mobility, excludes them from, or at best places them at the edge of, health delivery services. This study aimed to describe nomadic populations' characteristics, determine their perception on the current health services, and identify issues associated with community-based health interventions.
To develop a better health policy and strategic approaches adapted to nomadic populations, we conducted a cross-sectional study in the region of Timbuktu to describe the difficulties in accessing health services. The study consisted in administering questionnaires to community members in the communes of Ber and Gossi, in the Timbuktu region, to understand their perceptions of health services delivery in their settings.
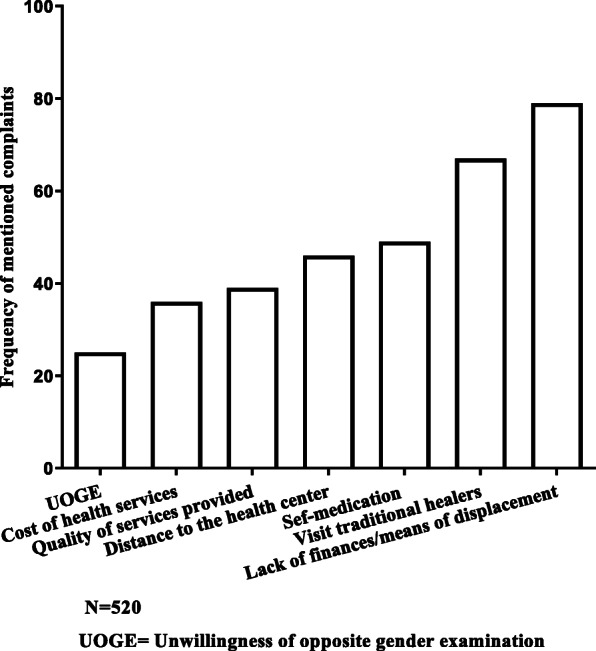
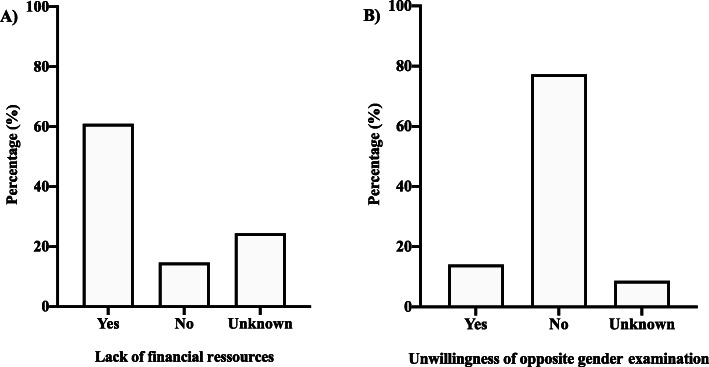
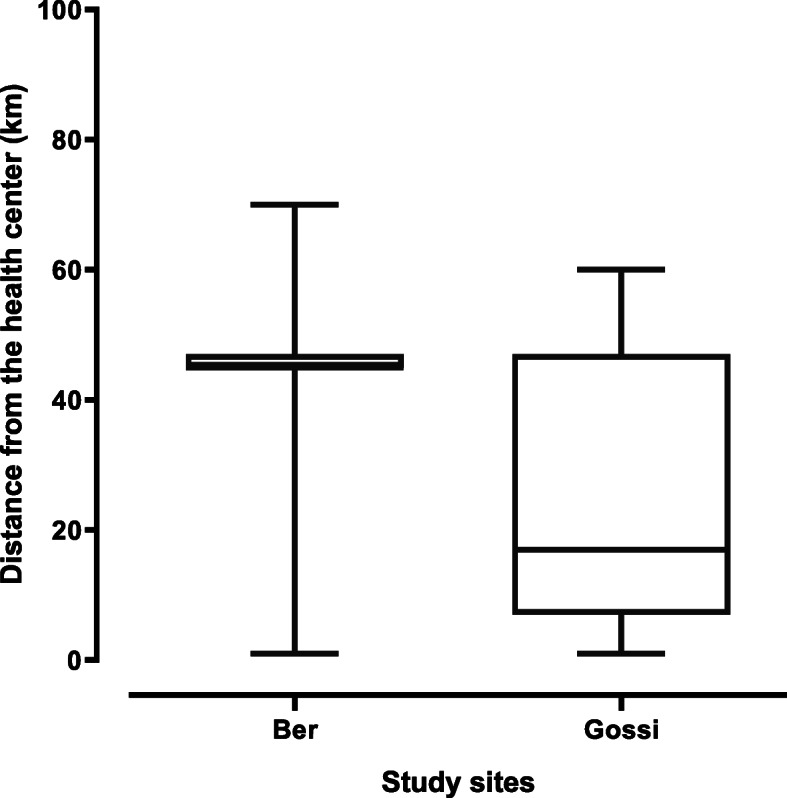
We interviewed 520 individuals, all members of the nomadic communities of the two study communes. Their median age was 38 years old with extremes ranging from 18 to 86 years old. Their main activities were livestock breeding (27%), housekeeping (26.4%), local trading (11%), farming (6%) and artisans (5.5%). The average distance to the local health center was 40.94 km and 23.19 km respectively in Gossi and Ber. In terms of barriers to access to health care, participants complained mainly about the transportation options (79.4%), the quality of provided services (39.2%) and the high cost of available health services (35.7%). Additionally, more than a quarter of our participants stated that they would not allow themselves to be examined by a health care worker of the opposite gender.
This study shows that nomadic populations do not have access to community-based health interventions. A number of factors were revealed to be important barriers per these communities' perception including the quality of services, poverty, lifestyle, gender and current health policy strategies in the region. To be successful, future interventions should take these factors into account by adapting policies and methods.
在马里,游牧人口分布在三分之一的领土上。他们的生活方式以不断迁移为特点,使他们无法获得或最多只能边缘性地获得卫生服务。本研究旨在描述游牧人口的特征,了解他们对当前卫生服务的看法,并确定与以社区为基础的卫生干预相关的问题。
为了制定更好的适应游牧人口的卫生政策和战略方法,我们在廷巴克图地区进行了一项横断面研究,以描述获得卫生服务的困难。该研究包括在廷巴克图地区的贝尔和戈西两个社区向社区成员发放问卷,以了解他们对所在环境卫生服务提供的看法。
我们共采访了 520 人,他们均为两个研究社区游牧社区的成员。他们的中位数年龄为 38 岁,极值为 18 至 86 岁。他们的主要活动是畜牧业(27%)、家务(26.4%)、本地贸易(11%)、农业(6%)和工匠(5.5%)。戈西和贝尔的当地卫生中心的平均距离分别为 40.94 公里和 23.19 公里。在获得医疗保健的障碍方面,参与者主要抱怨交通选择(79.4%)、提供服务的质量(39.2%)和现有卫生服务的高费用(35.7%)。此外,超过四分之一的参与者表示,他们不会允许卫生工作者为他们提供性别相反的体检。
本研究表明,游牧人口无法获得以社区为基础的卫生干预。根据这些社区的看法,一些因素被认为是重要的障碍,包括服务质量、贫困、生活方式、性别以及该地区当前的卫生政策策略。为了取得成功,未来的干预措施应考虑到这些因素,调整政策和方法。