Imajo Kento, Tetlow Louise, Dennis Andrea, Shumbayawonda Elizabeth, Mouchti Sofia, Kendall Timothy J, Fryer Eve, Yamanaka Shogi, Honda Yasushi, Kessoku Takaomi, Ogawa Yuji, Yoneda Masato, Saito Satoru, Kelly Catherine, Kelly Matt D, Banerjee Rajarshi, Nakajima Atsushi
Department of Gastroenterology and Hepatology, Yokohama City University School of Medicine, Yokohama 236-0004, Japan.
Innovation, Perspectum, Oxford OX4 2LL, United Kingdom.
World J Gastroenterol. 2021 Feb 21;27(7):609-623. doi: 10.3748/wjg.v27.i7.609.
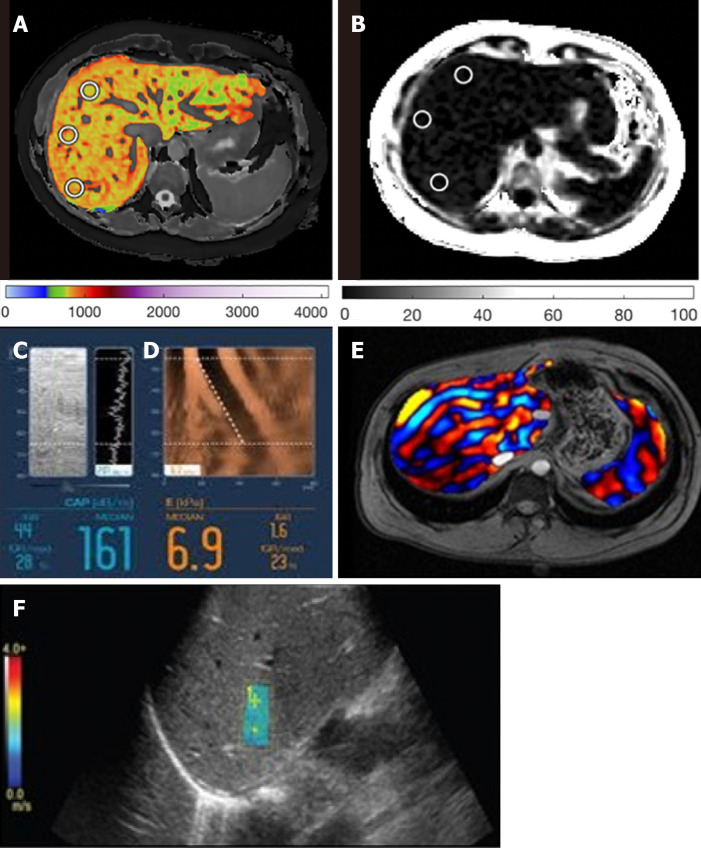
Non-invasive assessment of non-alcoholic steatohepatitis (NASH) is increasing in desirability due to the invasive nature and costs associated with the current form of assessment; liver biopsy. Quantitative multiparametric magnetic resonance imaging (mpMRI) to measure liver fat (proton density fat fraction) and fibroinflammatory disease [iron-corrected T1 (cT1)], as well as elastography techniques [vibration-controlled transient elastography (VCTE) liver stiffness measure], magnetic resonance elastography (MRE) and 2D Shear-Wave elastography (SWE) to measure stiffness and fat (controlled attenuated parameter, CAP) are emerging alternatives which could be utilised as safe surrogates to liver biopsy.
To evaluate the agreement of non-invasive imaging modalities with liver biopsy, and their subsequent diagnostic accuracy for identifying NASH patients.
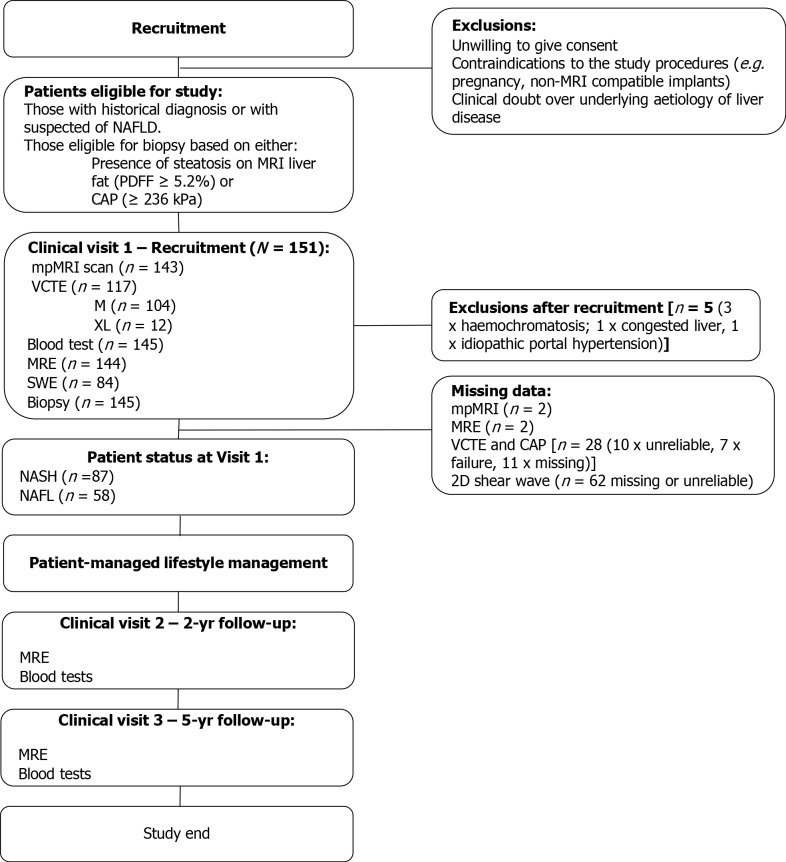
From January 2019 to February 2020, Japanese patients suspected of NASH were recruited onto a prospective, observational study and were screened using non-invasive imaging techniques; mpMRI with Liver , VCTE, MRE and 2D-SWE. Patients were subsequently biopsied, and samples were scored by three independent pathologists. The diagnostic performances of the non-invasive imaging modalities were assessed using area under receiver operating characteristic curve (AUC) with the median of the histology scores as the gold standard diagnoses. Concordance between all three independent pathologists was further explored using Krippendorff's alpha (a) from weighted kappa statistics.
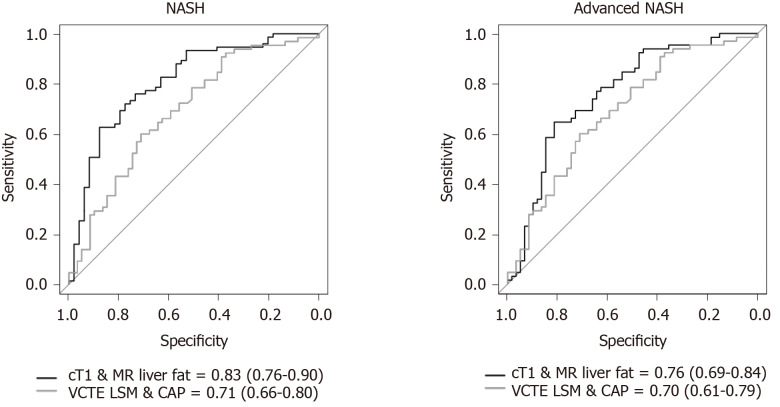
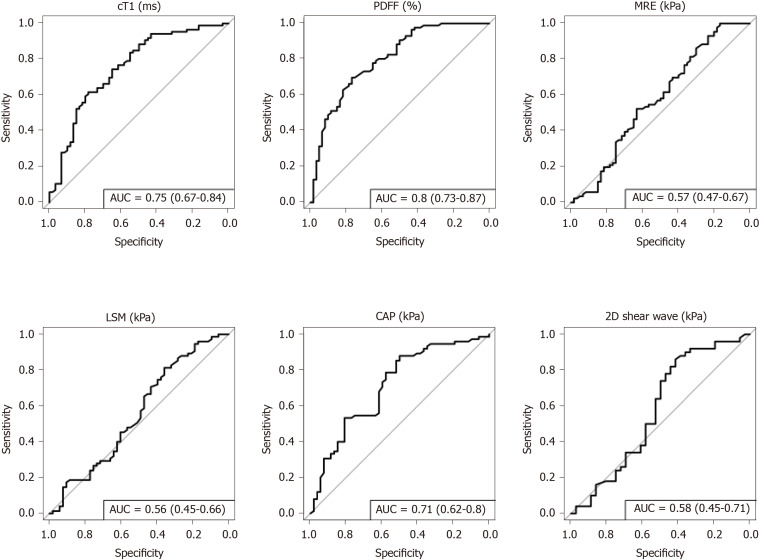
= 145 patients with mean age of 60 (SD: 13 years.), 39% females, and 40% with body mass index ≥ 30 kg/m were included in the analysis. For identifying patients with NASH, MR liver fat and cT1 were the strongest performing individual measures (AUC: 0.80 and 0.75 respectively), and the mpMRI metrics combined (cT1 and MR liver fat) were the overall best non-invasive test (AUC: 0.83). For identifying fibrosis ≥ 1, MRE performed best (AUC: 0.97), compared to VCTE-liver stiffness measure (AUC: 0.94) and 2D-SWE (AUC: 0.94). For assessment of steatosis ≥ 1, MR liver fat was the best performing non-invasive test (AUC: 0.92), compared to controlled attenuated parameter (AUC: 0.75). Assessment of the agreement between pathologists showed that concordance was best for steatosis (a = 0.58), moderate for ballooning (a = 0.40) and fibrosis (a = 0.40), and worst for lobular inflammation (a = 0.11).
Quantitative mpMRI is an effective alternative to liver biopsy for diagnosing NASH and non-alcoholic fatty liver, and thus may offer clinical utility in patient management.
由于当前非酒精性脂肪性肝炎(NASH)评估方式(肝活检)具有侵入性且成本较高,对其进行非侵入性评估的需求日益增加。定量多参数磁共振成像(mpMRI)用于测量肝脏脂肪(质子密度脂肪分数)和纤维炎症性疾病[铁校正T1(cT1)],以及弹性成像技术[振动控制瞬时弹性成像(VCTE)肝脏硬度测量]、磁共振弹性成像(MRE)和二维剪切波弹性成像(SWE)用于测量硬度和脂肪(受控衰减参数,CAP),这些新兴的替代方法可作为肝活检的安全替代指标。
评估非侵入性成像方式与肝活检的一致性,以及它们随后识别NASH患者的诊断准确性。
从2019年1月至2020年2月,将疑似NASH的日本患者纳入一项前瞻性观察性研究,并使用非侵入性成像技术进行筛查;使用肝脏专用mpMRI、VCTE、MRE和二维SWE。随后对患者进行活检,样本由三名独立病理学家评分。使用受试者操作特征曲线下面积(AUC)评估非侵入性成像方式的诊断性能,以组织学评分的中位数作为金标准诊断。使用加权kappa统计中的Krippendorff's alpha(α)进一步探讨所有三名独立病理学家之间的一致性。
分析纳入了145例患者,平均年龄60岁(标准差:13岁),39%为女性,40%体重指数≥30kg/m²。对于识别NASH患者,磁共振肝脏脂肪和cT1是表现最强的单项指标(AUC分别为0.80和0.75),并且mpMRI指标联合使用(cT1和磁共振肝脏脂肪)是总体最佳的非侵入性检查(AUC:0.83)。对于识别纤维化≥1,MRE表现最佳(AUC:0.97),相比之下VCTE肝脏硬度测量(AUC:0.94)和二维SWE(AUC:0.94)。对于评估脂肪变性≥1,磁共振肝脏脂肪是表现最佳的非侵入性检查(AUC:0.92),相比之下受控衰减参数(AUC:0.75)。对病理学家之间一致性的评估表明,脂肪变性的一致性最佳(α = 0.58),气球样变(α = 0.40)和纤维化(α = 0.40)的一致性中等,小叶炎症的一致性最差(α = 0.11)。
定量mpMRI是诊断NASH和非酒精性脂肪肝的有效替代肝活检的方法,因此可能在患者管理中具有临床应用价值。