Joseph A P, Newey A, Glover A, Mohabbat W
Emergency Department and Trauma Service, Royal North Shore Hospital, St Leonards, NSW 2065, Australia.
Radiology Department, Royal North Shore Hospital, St Leonards, NSW 2065, Australia.
Trauma Case Rep. 2021 Feb 9;32:100402. doi: 10.1016/j.tcr.2021.100402. eCollection 2021 Apr.
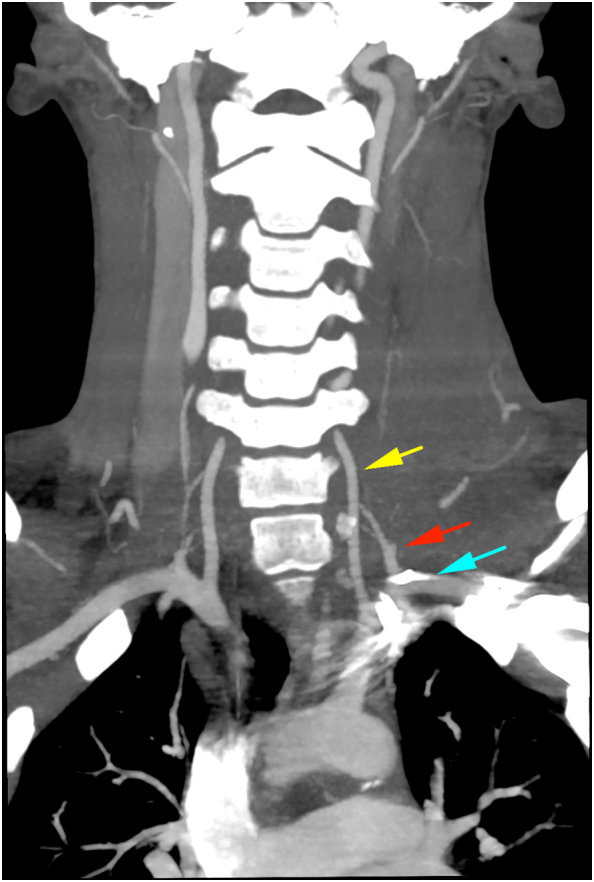
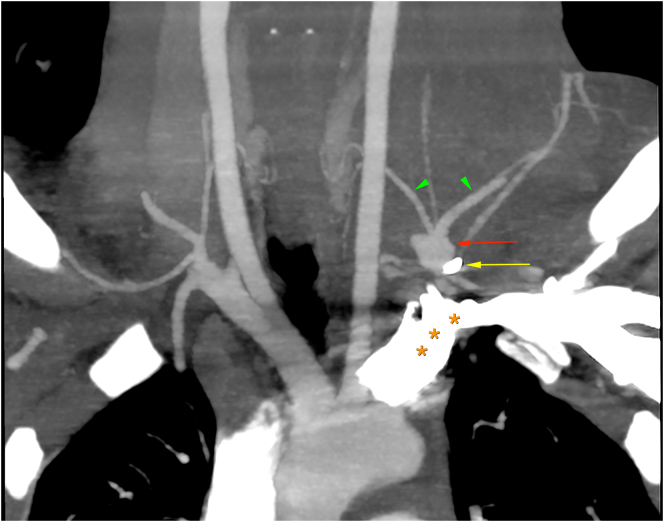
We present an unusual case of a young male with a penetrating neck injury (PNI) due to a work-related injury. A metallic foreign body traversed from entry at surgical Zone 2 to Zone 1 in the neck and resulted in a transection of the left thyrocervical trunk at the origin with the left subclavian artery. Computed Tomographic Angiography (CTA) of the aortic arch and major branch vessels demonstrated haemorrhage anterior to the left subclavian artery and left thyrocervical trunk. We describe some of the diagnostic and operative challenges which may occur in these rare and life-threatening injuries. We have also reviewed some of the recent key literature on this topic and have collated the recommendations of the review. In recent years, there has been a movement away from selective "zone-based" mandatory surgical exploration for Zone 2 injuries, as well as invasive and time-consuming investigations (such as digital subtraction angiography, contrast oesophageal swallow and bronchoscopy) for Zone 1 and 3 injuries due to the high number of negative surgical procedures and investigations. We demonstrate there is now an evidence-based algorithm which demonstrates that a "no zone" approach to the management of these patients is safe and effective. This requires an initial physical examination looking for the presence or absence of "hard", "soft" or "no" physical signs in these patients, and then deciding on subsequent management which would include immediate surgery, CTA of the aortic arch and branches (and subsequent surgical or other management) or observation only. Our aim in describing this case it to highlight that there is now good evidence-based guidance for the safe and effective management of patients with this infrequent but potentially fatal injury.
我们报告了一例因工作相关损伤导致穿透性颈部损伤(PNI)的年轻男性的罕见病例。一个金属异物从颈部手术2区的入口穿过至1区,导致左甲状腺颈干在起始处与左锁骨下动脉横断。主动脉弓及主要分支血管的计算机断层血管造影(CTA)显示左锁骨下动脉和左甲状腺颈干前方有出血。我们描述了这些罕见且危及生命的损伤可能出现的一些诊断和手术挑战。我们还回顾了近期关于该主题的一些关键文献,并整理了综述的建议。近年来,由于阴性手术和检查数量众多,对于2区损伤已不再采用选择性“分区”强制性手术探查,对于1区和3区损伤也不再进行侵入性且耗时的检查(如数字减影血管造影、食管造影和支气管镜检查)。我们证明现在有一种基于证据的算法,表明对这些患者采用“无分区”管理方法是安全有效的。这需要进行初步体格检查,查看这些患者是否存在“硬”、“软”或“无”体征,然后决定后续管理措施,包括立即手术、主动脉弓及分支的CTA(以及后续手术或其他管理)或仅观察。我们描述此病例的目的是强调,对于这种不常见但可能致命的损伤患者的安全有效管理,现在有很好的基于证据的指导。