Meyer Charles, Anderson Danielle, Dong Zhiqiao, Riddick Jeanelle Braxton, Elrod Marilisa, Ayala Marco
Department of Otolaryngology-Head and Neck Surgery, Naval Medical Center Portsmouth, Portsmouth, Virginia, USA.
Department of Pediatrics, Naval Medical Center Portsmouth, Portsmouth, Virginia, USA.
OTO Open. 2021 Feb 16;5(1):2473974X21992001. doi: 10.1177/2473974X21992001. eCollection 2021 Jan-Mar.
Following thyroid lobectomy, patients are at risk for hypothyroidism. This study sought to determine the incidence of postlobectomy thyroid hormone replacement as well as predictive risk factors to better counsel patients.
Retrospective cohort study.
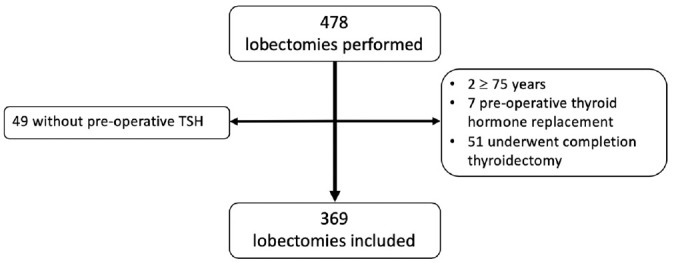
Patients aged 18 to 75 years treated in a single academic institution who underwent thyroid lobectomy from October 2006 to September 2017.
Patients were followed for an average of 73 months. Demographic data, body mass index, size of removed and remnant lobe, preoperative thyroid-stimulating hormone (TSH) level, final thyroid pathology, and presence of thyroiditis were collected and analyzed. Risk factors were evaluated with chi-square analyses, tests, logistic regression, and Kaplan-Meier analysis.
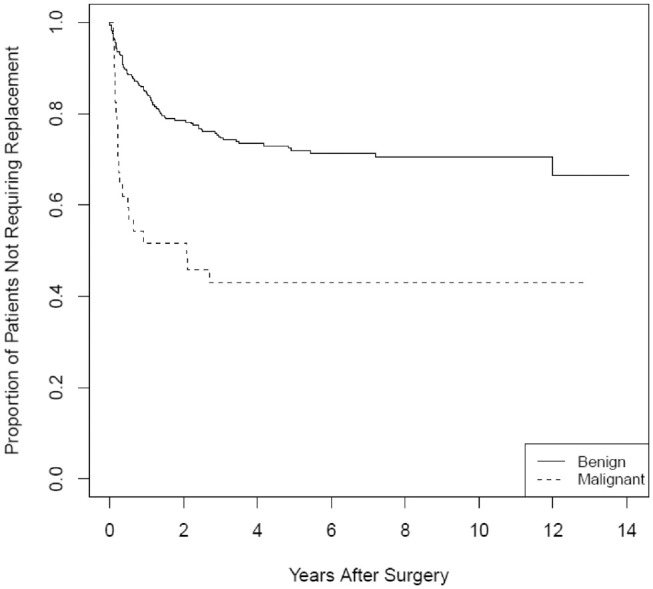
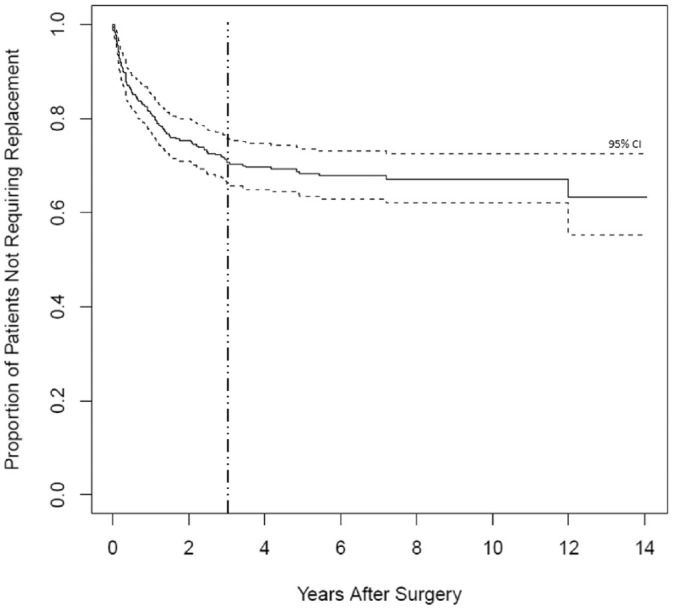
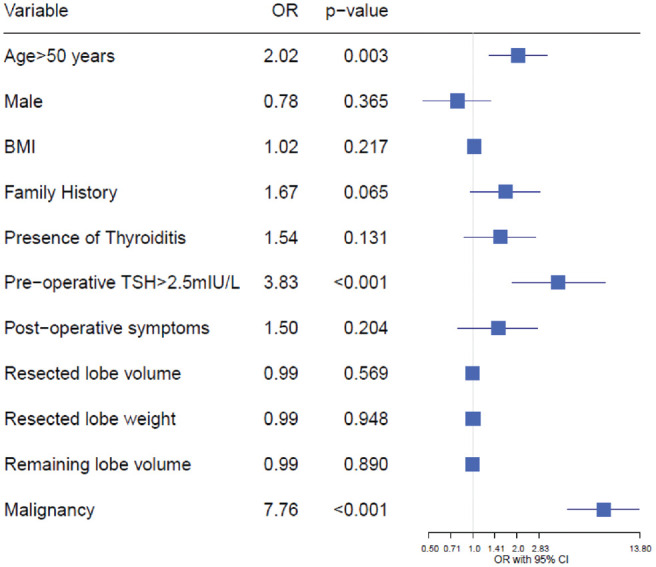
Of the 478 patients reviewed, 369 were included in the analysis, 30% of whom eventually required thyroid hormone replacement. More than 39% started therapy >12 months postoperatively, with 90% treated within 36 months. Patient age ≥50 years and preoperative TSH ≥2.5 mIU/L were associated with odds ratios of 2.034 and 3.827, respectively, for thyroid hormone replacement. Malignancy on final pathology demonstrated an odds ratio of 7.76 for hormone replacement. Sex, body mass index, volume of resected and remaining lobes, and weight of resected lobe were not significant predictors.
Nearly a third of patients may ultimately require thyroid hormone replacement. Age at the time of surgery, preoperative TSH, and final pathology are strong, clinically relevant predictors of the need for future thyroid hormone replacement. After lobectomy, patients should have long-term thyroid function follow-up to monitor for delayed hypothyroidism.
甲状腺叶切除术后,患者存在甲状腺功能减退的风险。本研究旨在确定甲状腺叶切除术后甲状腺激素替代治疗的发生率以及预测风险因素,以便更好地为患者提供咨询。
回顾性队列研究。
2006年10月至2017年9月在一家学术机构接受甲状腺叶切除术的18至75岁患者。
对患者平均随访73个月。收集并分析人口统计学数据、体重指数、切除叶和残留叶的大小、术前促甲状腺激素(TSH)水平、最终甲状腺病理结果以及甲状腺炎的存在情况。通过卡方分析、检验、逻辑回归和Kaplan-Meier分析评估风险因素。
在审查的478例患者中,369例纳入分析,其中30%最终需要甲状腺激素替代治疗。超过39%的患者在术后12个月以上开始治疗,90%在36个月内接受治疗。患者年龄≥50岁和术前TSH≥2.5 mIU/L与甲状腺激素替代治疗的比值比分别为2.034和3.827。最终病理显示恶性肿瘤的激素替代治疗比值比为7.76。性别、体重指数、切除叶和残留叶的体积以及切除叶的重量不是显著的预测因素。
近三分之一的患者最终可能需要甲状腺激素替代治疗。手术时的年龄、术前TSH和最终病理结果是未来甲状腺激素替代治疗需求的强有力的、临床相关的预测因素。甲状腺叶切除术后,患者应进行长期甲状腺功能随访,以监测迟发性甲状腺功能减退。