Department of Infectious Diseases, Aarhus University Hospital, Aarhus N, Denmark.
Gilead Sciences Denmark, Copenhagen S, Denmark.
HIV Med. 2021 Jul;22(6):478-490. doi: 10.1111/hiv.13077. Epub 2021 Feb 28.
To estimate the burden of non-communicable diseases (NCDs) and mortality among PLHIV in the pre-, early- and late-HAART (highly active antiretroviral therapy) era.
We conducted a cohort study using population-based Danish medical registries including all adult HIV-infected residents of the Central Denmark Region during 1985-2017. For each HIV patient, we selected 10 comparisons from the background population matched by age, sex and municipality of residence. Based on hospital-related diagnoses we estimated the prevalence and incidence of specific NCD at diagnosis and at 5 and 10 years.
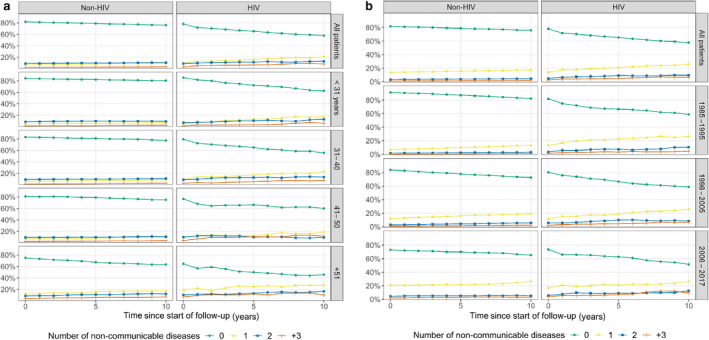
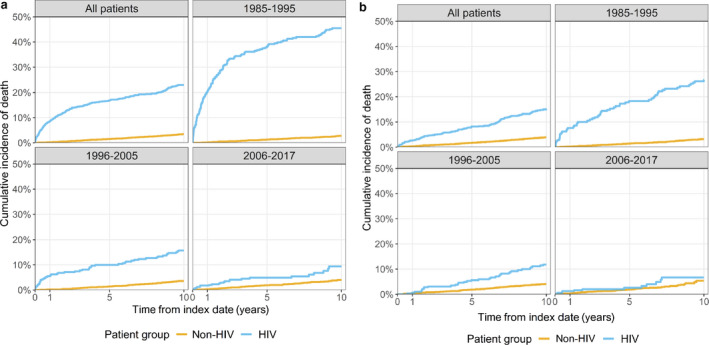
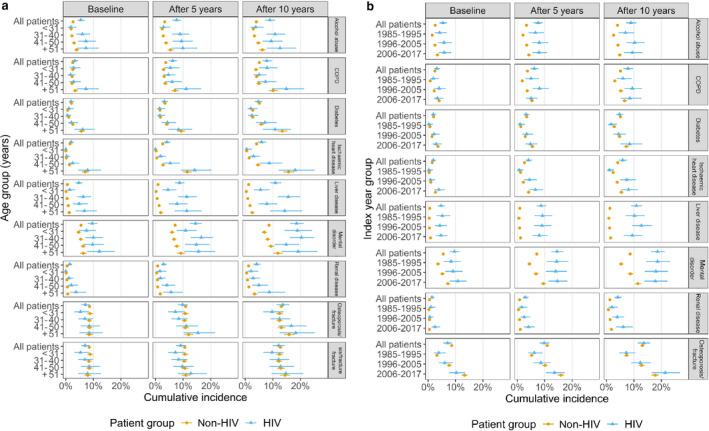
We identified 1043 PLHIV and 10 430 matched comparisons. PLHIV had lower socioeconomic status and more were born outside western Europe. At HIV diagnosis, 21.9% of PHLIV vs. 18.2% of non-HIV individuals had at least one NCD, increasing to 42.2% vs. 25.9% after 10 years. PLHIV had higher prevalence and cumulative incidence of alcohol abuse, chronic obstructive pulmonary disease (COPD), ischaemic heart disease, mental disorders, renal and liver disease, but no increased risk of diabetes mellitus. Only PLHIV in the age groups 41-50 and > 51 years had an increased incidence of osteoporosis. From the pre- to the late-HAART era, 10-year mortality among PLHIV decreased from 45.5% to 9.4% but continued at more than twice that of uninfected comparisons. However, in the late-HAART era, the mortality of PLHIV who were alive 2 years after HIV diagnosis was approaching that of comparisons.
Even in the late-HAART era, PLHIV have an excess mortality, which may be attributable to several NCDs being more prevalent among PLHIV. The prevalence rates of ischaemic heart disease, diabetes, osteoporosis and renal disease tend to increase over calendar time. Therefore, improvement of survival and quality of life of PLHIV neets strategies to reduce the risk of developing NCDs, including avoiding toxic antiretroviral therapy and lifestyle changes.
估计在高效抗逆转录病毒治疗(highly active antiretroviral therapy,HAART)前、早期和晚期时代,艾滋病毒感染者(people living with HIV,PLHIV)中的非传染性疾病(non-communicable diseases,NCD)负担和死亡率。
我们使用基于人群的丹麦医学登记处进行了一项队列研究,该登记处包括丹麦中部地区所有成年艾滋病毒感染者居民,时间为 1985 年至 2017 年。对于每一位 HIV 患者,我们从背景人群中选择了 10 名年龄、性别和居住地相匹配的对照者。基于与医院相关的诊断,我们估计了在诊断时以及 5 年和 10 年后特定 NCD 的患病率和发病率。
我们确定了 1043 名 PLHIV 和 10430 名匹配对照者。PLHIV 的社会经济地位较低,且更多人出生于西欧以外地区。在 HIV 诊断时,21.9%的 PLHIV 与 18.2%的非 HIV 个体至少有一种 NCD,10 年后这一比例分别增加到 42.2%和 25.9%。PLHIV 的酒精滥用、慢性阻塞性肺疾病(chronic obstructive pulmonary disease,COPD)、缺血性心脏病、精神障碍、肾脏和肝脏疾病的患病率和累积发病率更高,但糖尿病的风险没有增加。只有 41-50 岁和>51 岁的 PLHIV 骨质疏松症的发病率增加。从 HAART 前时代到晚期时代,PLHIV 的 10 年死亡率从 45.5%下降到 9.4%,但仍高于未感染对照者的两倍以上。然而,在晚期 HAART 时代,HIV 诊断后存活 2 年的 PLHIV 的死亡率接近对照者。
即使在晚期 HAART 时代,PLHIV 的死亡率仍然过高,这可能归因于 PLHIV 中更普遍存在的几种 NCD。缺血性心脏病、糖尿病、骨质疏松症和肾脏疾病的患病率趋势随时间而增加。因此,改善 PLHIV 的生存和生活质量需要采取策略来降低 NCD 的风险,包括避免有毒的抗逆转录病毒治疗和生活方式的改变。