Schukow Casey, Nordyke Billy R
Michigan State University College of Osteopathic Medicine.
Henry Ford Health System.
Spartan Med Res J. 2020 Oct 30;5(2):17738. doi: 10.51894/001c.17738.
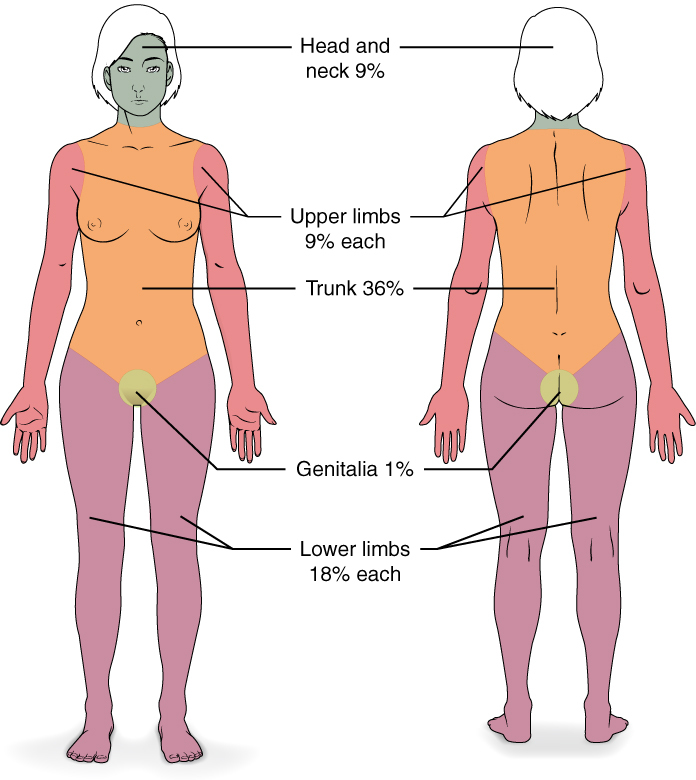
Although pressure cookers are very common kitchen utensils used in the United States, only a few cases of serious injuries secondary to pressure cooker explosions have been reported in the medical literature. When second-degree (i.e., "partial-thickness") burns result from pressure cooker explosions, wounds involving near to or greater than 10% of total body surface area typically require multidisciplinary treatment, with burn center referral for proper wound care, potential fluid resuscitation, and eventual scar management.
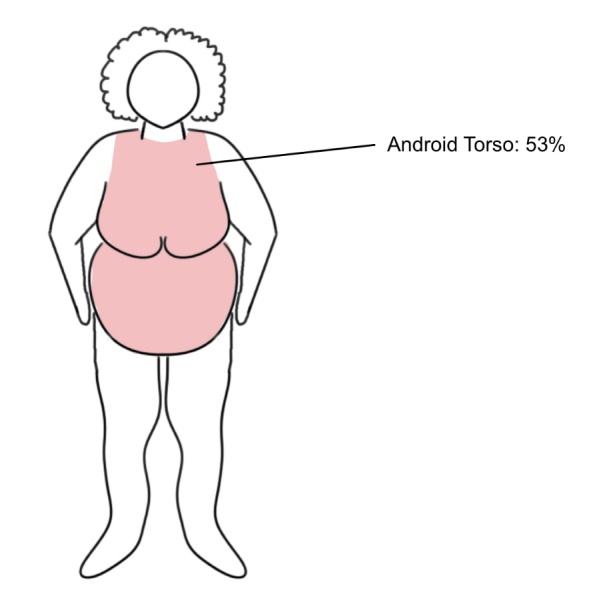
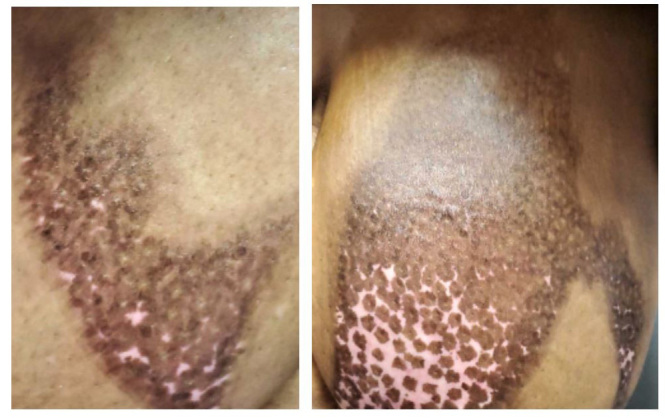
The example patient described in this report was an African American female in her early 30s who presented during the summer of 2020 after suffering varying levels of second-degree burns to her bilateral upper torso and left wrist (i.e., approximately 10%, total body surface area). The authors first saw the patient during a primary care office visit a week after her initial injury when she first went to a local urgent care clinic. Upon her arrival to the second author's family medicine clinic, a multi-specialty wound recovery plan was initiated since her first urgent care visit treatment had been minimal without prophylactic antibiotic therapy or placement of a burn center referral.
Partial and full-thickness burn injuries generally warrant immediate clinical (i.e., body surface area burn assessment, fluid resuscitation, empiric antibiotics) as well as ongoing (burn center referral, debridement procedures, active scar management, provision of psychological support) treatment needs. This paper discusses the critical opportunities posed for more extensive burn patients' physicians to first categorize the extent of burn wounds and initiate subsequent specialty care in other settings.
尽管高压锅在美国是非常常见的厨房用具,但医学文献中仅报道了少数几例因高压锅爆炸导致严重受伤的病例。当高压锅爆炸导致二度(即“部分厚度”)烧伤时,伤口累及近10%或超过全身表面积的10%时,通常需要多学科治疗,转诊至烧伤中心以获得适当的伤口护理、可能的液体复苏以及最终的瘢痕管理。
本报告中描述的示例患者是一名30岁出头的非裔美国女性,2020年夏天就诊,双侧上半身和左手腕有不同程度的二度烧伤(即约占全身表面积的10%)。作者在患者初次受伤一周后,她首次前往当地紧急护理诊所时,在一次初级保健门诊中首次见到该患者。在她来到第二作者的家庭医学诊所时,由于她首次在紧急护理诊所的治疗非常有限,没有预防性抗生素治疗或转诊至烧伤中心,因此启动了一个多专科伤口恢复计划。
部分厚度和全厚度烧伤通常需要立即进行临床治疗(即烧伤面积评估、液体复苏、经验性抗生素治疗)以及持续治疗(转诊至烧伤中心、清创手术、积极的瘢痕管理、提供心理支持)。本文讨论了对于更广泛烧伤患者的医生来说,首先对烧伤伤口的程度进行分类并在其他环境中启动后续专科护理所面临的关键机遇。