Emergency Department, CHU Angers, Institut Mitovasc UMR (CNRS 6015-INSERM 1083), UNIV Angers, F-CRIN INNOVTE, Angers, France.
Emergency Department, CHU Angers, Angers, France.
JAMA Cardiol. 2021 Jun 1;6(6):669-677. doi: 10.1001/jamacardio.2021.0064.
In patients with suspected pulmonary embolism (PE), overuse of diagnostic imaging is an important point of concern.
To derive and validate a 4-level pretest probability rule (4-Level Pulmonary Embolism Clinical Probability Score [4PEPS]) that makes it possible to rule out PE solely on clinical criteria and optimized D-dimer measurement to safely decrease imaging testing for suspected PE.
DESIGN, SETTING, AND PARTICIPANTS: This study included consecutive outpatients suspected of having PE from US and European emergency departments. Individual data from 3 merged management studies (n = 11 114; overall prevalence of PE, 11%) were used for the derivation cohort and internal validation cohort. The external validation cohorts were taken from 2 independent studies, the first with a high PE prevalence (n = 1548; prevalence, 21.5%) and the second with a moderate PE prevalence (n = 1669; prevalence, 11.7%). A prior definition of pretest probability target values to achieve a posttest probability less than 2% was used on the basis of the negative likelihood ratios of D-dimer. Data were collected from January 2003 to April 2016, and data were analyzed from June 2018 to August 2019.
The rate of PE diagnosed during the initial workup or during follow-up and the rate of imaging testing.
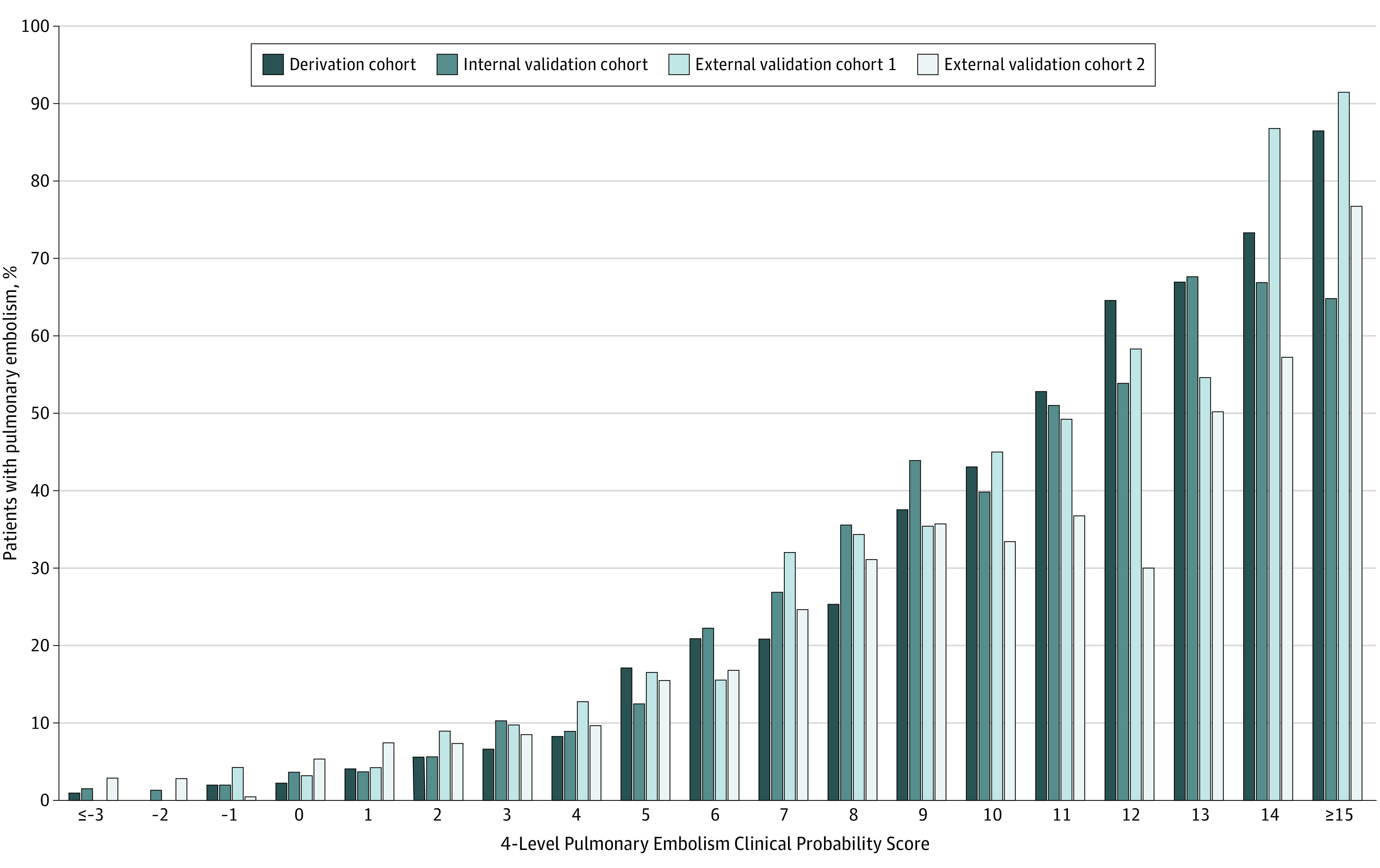
Of the 5588 patients in the derivation cohort, 3441 (61.8%) were female, and the mean (SD) age was 52 (18.5) years. The 4PEPS comprises 13 clinical variables scored from -2 to 5. It results in the following strategy: (1) very low probability of PE if 4PEPS is less than 0: PE ruled out without testing; (2) low probability of PE if 4PEPS is 0 to 5: PE ruled out if D-dimer level is less than 1.0 μg/mL; (3) moderate probability of PE if 4PEPS is 6 to 12: PE ruled out if D-dimer level is less than the age-adjusted cutoff value; (4) high probability of PE if 4PEPS is greater than 12: PE ruled out by imaging without preceding D-dimer test. In the first and the second external validation cohorts, the area under the receiver operator characteristic curves were 0.79 (95% CI, 0.76 to 0.82) and 0.78 (95% CI, 0.74 to 0.81), respectively. The false-negative testing rates if the 4PEPS strategy had been applied were 0.71% (95% CI, 0.37 to 1.23) and 0.89% (95% CI, 0.53 to 1.49), respectively. The absolute reductions in imaging testing were -22% (95% CI, -26 to -19) and -19% (95% CI, -22 to -16) in the first and second external validation cohorts, respectively. The 4PEPS strategy compared favorably with all recent strategies in terms of imaging testing.
The 4PEPS strategy may lead to a substantial and safe reduction in imaging testing for patients with suspected PE. It should now be tested in a formal outcome study.
在疑似肺栓塞(PE)患者中,过度使用诊断性影像学检查是一个重要的关注点。
制定并验证一个 4 级预测概率规则(4-Level Pulmonary Embolism Clinical Probability Score [4PEPS]),该规则可仅根据临床标准和优化的 D-二聚体测量结果排除 PE,从而安全减少疑似 PE 的影像学检查。
设计、地点和参与者:这项研究纳入了来自美国和欧洲急诊科的连续疑似患有 PE 的门诊患者。来自 3 项合并管理研究的个体数据(n = 11 114;PE 的总体患病率为 11%)用于推导队列和内部验证队列。外部验证队列来自 2 项独立研究,其中第一项研究的 PE 患病率较高(n = 1548;患病率为 21.5%),第二项研究的 PE 患病率中等(n = 1669;患病率为 11.7%)。根据 D-二聚体的负似然比,采用预先定义的预测概率目标值来排除检测后概率小于 2%。数据收集于 2003 年 1 月至 2016 年 4 月,数据分析于 2018 年 6 月至 2019 年 8 月进行。
在初始检查或随访期间诊断为 PE 的比例以及影像学检查的比例。
在推导队列的 5588 名患者中,3441 名(61.8%)为女性,平均(SD)年龄为 52(18.5)岁。4PEPS 包含 13 个从-2 到 5 分的临床变量。它产生了以下策略:(1)如果 4PEPS 小于 0,则 PE 的可能性非常低:如果 D-二聚体水平小于 1.0μg/mL,则无需检测即可排除 PE;(2)如果 4PEPS 为 0 至 5,则 PE 的可能性较低:如果 D-二聚体水平小于年龄调整后的临界值,则排除 PE;(3)如果 4PEPS 为 6 至 12,则 PE 的可能性为中度:如果 D-二聚体水平小于年龄调整的临界值,则排除 PE;(4)如果 4PEPS 大于 12,则 PE 的可能性较高:如果没有事先进行 D-二聚体检测,则通过影像学检查排除 PE。在第一个和第二个外部验证队列中,受试者工作特征曲线下的面积分别为 0.79(95%CI,0.76 至 0.82)和 0.78(95%CI,0.74 至 0.81)。如果应用 4PEPS 策略,假阴性检测率分别为 0.71%(95%CI,0.37 至 1.23)和 0.89%(95%CI,0.53 至 1.49)。在第一个和第二个外部验证队列中,影像学检查的绝对减少率分别为-22%(95%CI,-26 至-19)和-19%(95%CI,-22 至-16)。就影像学检查而言,4PEPS 策略与最近的所有策略相比均具有优势。
4PEPS 策略可能会导致疑似 PE 患者的影像学检查大幅减少,且安全。现在应在正式的结局研究中进行检验。