Department of Primary Care and Public Health, Imperial College London.
The Dr Foster Unit, Department of Primary Care and Public Health, Imperial College London, London.
Br J Gen Pract. 2021 Jun 24;71(708):e547-e554. doi: 10.3399/BJGP.2020.0986. Print 2021 Jul.
In the UK, while most primary care contacts are uncomplicated, safety incidents do occur and result in patient harm, for example, failure to recognise a patient's deterioration in health.
To determine the patient and healthcare factors associated with potentially missed acute deterioration in health.
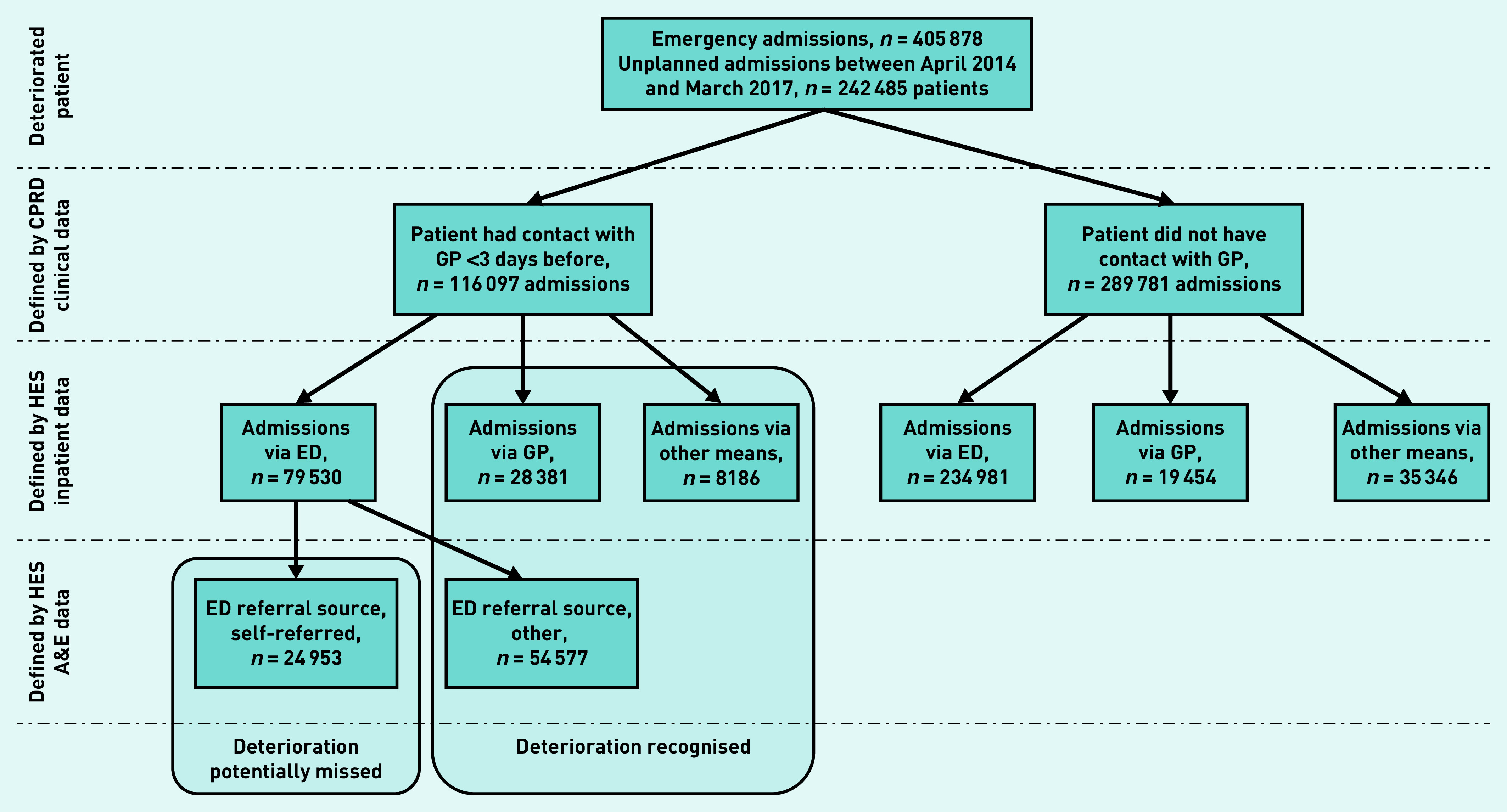
Cohort of patients registered with English Clinical Practice Research Datalink general practices between 1 April 2014 and 31 December 2017 with linked hospital data.
A potentially missed acute deterioration was defined as a patient having a self-referred admission to hospital having been seen in primary care by a GP in the 3 days beforehand. All diagnoses and subsets of commonly-reported missed conditions were analysed..
A total of 116 097 patients contacted a GP 3 days before an emergency admission. Patients with sepsis (adjusted odds ratio [aOR] 1.09, 95% confidence interval [CI] = 1.01 to 1.18) or urinary tract infections (aOR 1.09, 95% CI = 1.04 to 1.14) were more likely to self-refer. The duration of GP appointments was associated with self-referral. On average, a 5-minute increase in appointment time resulted in a 10% decrease in the odds of self-referred admissions (aOR 0.90, 95% CI = 0.89 to 0.91). Patients having a telephone consultation (compared with face-to-face consultation) (aOR 1.14, 95% CI = 1.11 to 1.18) previous health service use, and presence of comorbidities were also associated with self-referred admission.
Differentiating acute deterioration from self-limiting conditions can be difficult for clinicians, particularly in patients with sepsis, urinary tract infections, or long-term conditions. The findings of this study support the call for longer GP consultations and caution against reliance on telephone consultations in primary care; however, more research is needed to understand the underlying mechanisms.
在英国,虽然大多数初级保健接触都不复杂,但确实会发生安全事件并导致患者受到伤害,例如未能识别患者健康状况的恶化。
确定与潜在急性健康恶化相关的患者和医疗保健因素。
2014 年 4 月 1 日至 2017 年 12 月 31 日期间在英国临床实践研究数据链接普通实践中注册的患者队列,具有相关的医院数据。
潜在的急性恶化定义为患者在初级保健中由全科医生就诊后的 3 天内自行转诊住院。分析了所有诊断和常见漏诊疾病的子集。
共有 116097 名患者在紧急入院前 3 天联系了全科医生。患有败血症(调整后的优势比[OR]1.09,95%置信区间[CI]为 1.01 至 1.18)或尿路感染(OR 1.09,95%CI 为 1.04 至 1.14)的患者更有可能自行转诊。全科医生预约的持续时间与自行转诊有关。平均而言,预约时间增加 5 分钟,自行转诊的几率降低 10%(OR 0.90,95%CI 为 0.89 至 0.91)。与面对面咨询相比,进行电话咨询(OR 1.14,95%CI 为 1.11 至 1.18)、以前的卫生服务使用和并存疾病也与自行转诊入院相关。
对于临床医生来说,区分急性恶化与自限性疾病可能具有挑战性,特别是在患有败血症、尿路感染或长期疾病的患者中。本研究的结果支持呼吁延长全科医生咨询时间,并谨慎依赖初级保健中的电话咨询;然而,需要进一步研究以了解潜在机制。