Camara Bully, Oluwalana Claire, Miyahara Reiko, Lush Alyson, Kampmann Beate, Manneh Kebba, Okomo Uduak, D'Alessandro Umberto, Roca Anna
Medical Research Council Unit the Gambia at London School of Hygiene and Tropical Medicine, Banjul, Gambia.
Department of Clinical Tropical Medicine, Institute of Tropical Medicine, Graduate School of Tropical Medicine, Nagasaki University, Nagasaki, Japan.
Front Pediatr. 2021 Feb 15;9:579922. doi: 10.3389/fped.2021.579922. eCollection 2021.
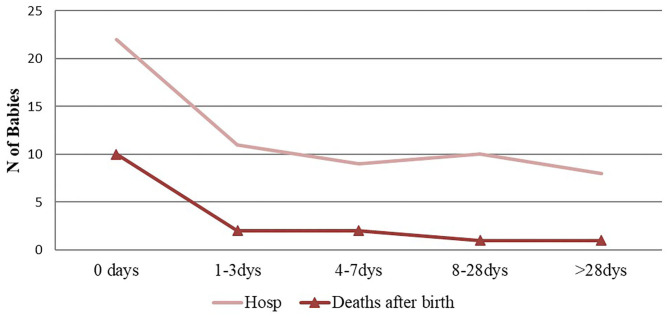
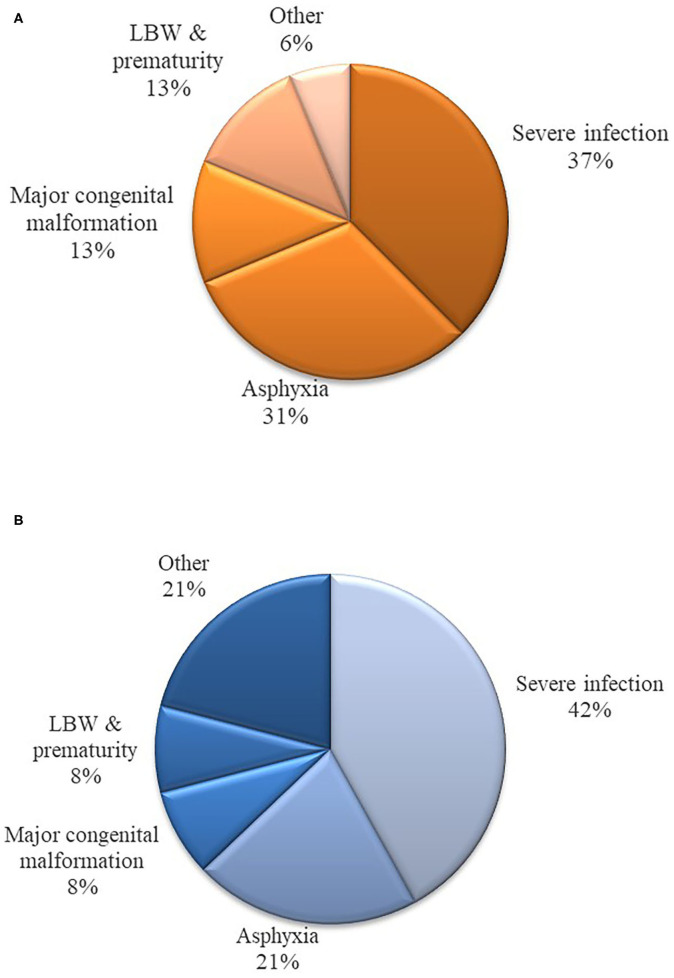
The Gambia Demographic and Health Survey 2013 data showed that up to 63% of deliveries in the country occur in health facilities. Despite such a high rate, there are few facility-based studies on delivery outcomes in the country. This analysis ancillary to a randomized control trial describes occurrence of poor pregnancy outcomes in a cohort of women and their infants delivering in a government health facility in urban Gambia. Using clinical information obtained during the trial, we calculated rates of poor pregnancy outcomes including stillbirths, hospitalization and neonatal deaths. Logistic regression was used to calculate odds ratio (OR) and 95% confidence interval (CI) in the risk factors analysis. Between April 2013 and 2014, 829 mothers delivered 843 babies, including 13 stillbirths [15.4 (7.1-23.8)] per 1,000 births. Among 830 live born infants, 7.6% ( = 63) required hospitalization during the 8-week follow-up period. Most of these hospitalizations (74.6%) occurred during the early neonatal period (<7 days of life). Severe clinical infections (i.e., sepsis, meningitis and pneumonia) ( = 27) were the most common diagnoses, followed by birth asphyxia ( = 13), major congenital malformations ( = 10), jaundice ( = 6) and low birth weight ( = 5). There were sixteen neonatal deaths, most of which also occurred during the early neonatal period. Overall, neonatal mortality rate (NMR) and perinatal mortality rate (PMR) were 19.3 (CI: 9.9-28.7) per 1,000 live births and 26.1 (CI: 15.3-36.9) per 1,000 total births, respectively. Severe clinical infections and birth asphyxia accounted for 37 and 31% of neonatal deaths, respectively. The risk of hospitalization was higher among neonates with severe congenital malformations, low birth weight, twin deliveries, and those born by cesarean section. Risk of mortality was higher among neonates with severe congenital malformations and twin deliveries. Neonatal hospitalization and deaths in our cohort were high. Although vertical interventions may reduce specific causes of morbidity and mortality, data indicate the need for a holistic approach to significantly improve the rates of poor pregnancy outcomes. Critically, a focus on decreasing the high rate of stillbirths is warranted. ClinicalTrials.gov Identifier: NCT01800942.
2013年冈比亚人口与健康调查数据显示,该国高达63%的分娩在医疗机构进行。尽管这一比例很高,但该国基于医疗机构的分娩结局研究却很少。这项作为随机对照试验辅助分析的研究描述了在冈比亚城市一家政府医疗机构分娩的一组妇女及其婴儿中不良妊娠结局的发生情况。利用试验期间获得的临床信息,我们计算了包括死产、住院和新生儿死亡在内的不良妊娠结局发生率。在风险因素分析中,采用逻辑回归计算比值比(OR)和95%置信区间(CI)。2013年4月至2014年期间,829名母亲分娩了843名婴儿,其中每1000例分娩中有13例死产[15.4(7.1 - 23.8)]。在830名活产婴儿中,7.6%(n = 63)在8周随访期内需要住院治疗。这些住院治疗大多(74.6%)发生在新生儿早期(出生后<7天)。严重临床感染(即败血症、脑膜炎和肺炎)(n = 27)是最常见的诊断,其次是出生窒息(n = 13)、重大先天性畸形(n = 10)、黄疸(n = 6)和低出生体重(n = 5)。有16例新生儿死亡,其中大多数也发生在新生儿早期。总体而言,每1000例活产的新生儿死亡率(NMR)和围产期死亡率(PMR)分别为19.3(CI:9.9 - 28.7)和每1000例总分娩26.1(CI:15.3 - 36.9)。严重临床感染和出生窒息分别占新生儿死亡的37%和31%。患有严重先天性畸形、低出生体重、双胎分娩以及剖宫产出生的新生儿住院风险更高。患有严重先天性畸形和双胎分娩的新生儿死亡风险更高。我们队列中的新生儿住院和死亡情况很严重。虽然纵向干预可能会降低特定的发病和死亡原因,但数据表明需要采取整体方法来显著改善不良妊娠结局的发生率。至关重要的是,有必要关注降低高死产率。临床试验注册号:NCT01800942。