Yokoshiki Hisashi, Shimizu Akihiko, Mitsuhashi Takeshi, Ishibashi Kohei, Kabutoya Tomoyuki, Yoshiga Yasuhiro, Kohno Ritsuko, Abe Haruhiko, Nogami Akihiko
Department of Cardiovascular Medicine Sapporo City General Hospital Sapporo Japan.
UBE Kohsan Central Hospital Upe Japan.
J Arrhythm. 2020 Nov 28;37(1):148-156. doi: 10.1002/joa3.12468. eCollection 2021 Feb.
The aim of this study was to clarify the current status and role of programmed ventricular stimulation in patients without sustained ventricular arrhythmias and reduced left ventricular ejection fraction (LVEF).
The follow-up data of the Japan cardiac device treatment registry (JCDTR) was analyzed in 746 patients with LVEF ≦35% and no prior history of sustained ventricular arrhythmias who underwent de novo implantable cardioverter-defibrillator (ICD) or cardiac resynchronization therapy with a defibrillator (CRT-D) implantation between January 2011 and August 2015.
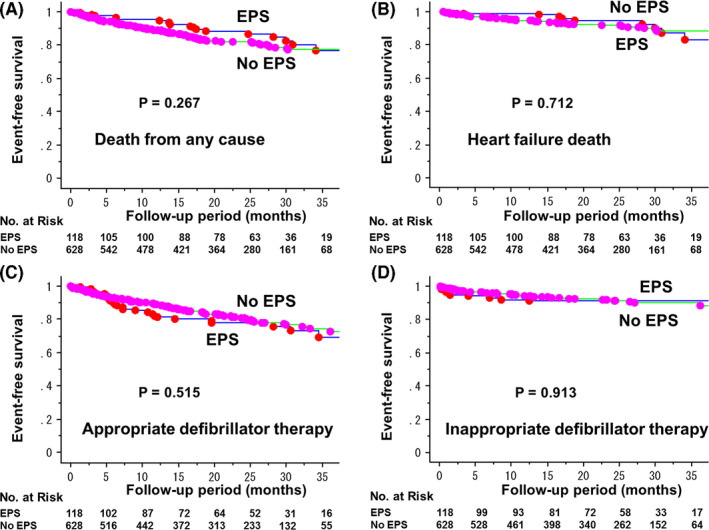
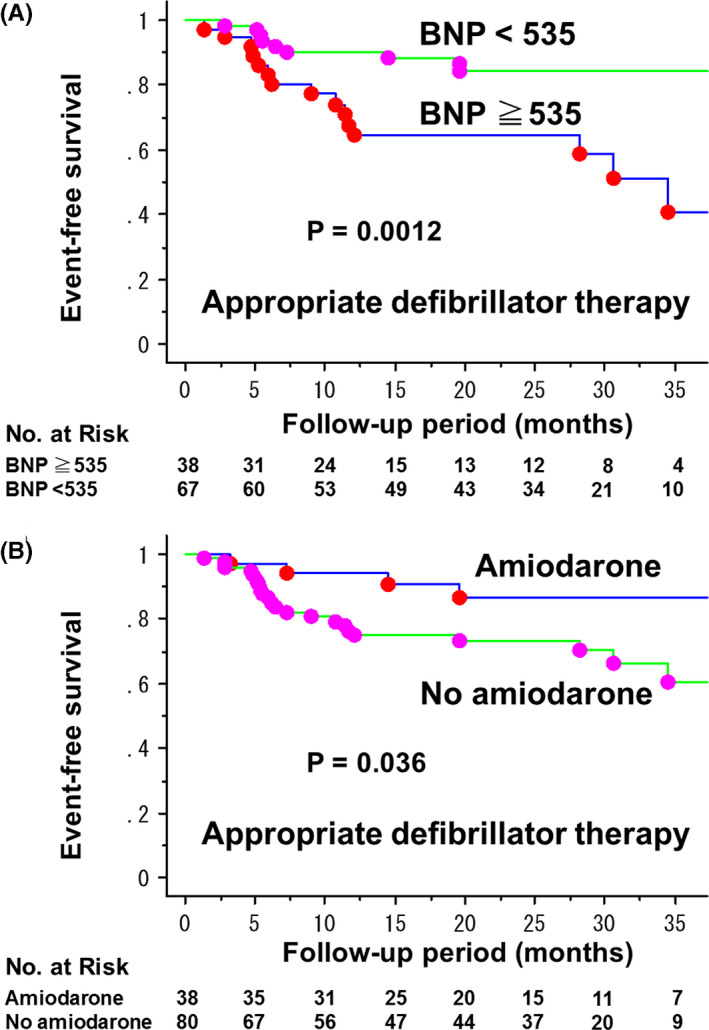
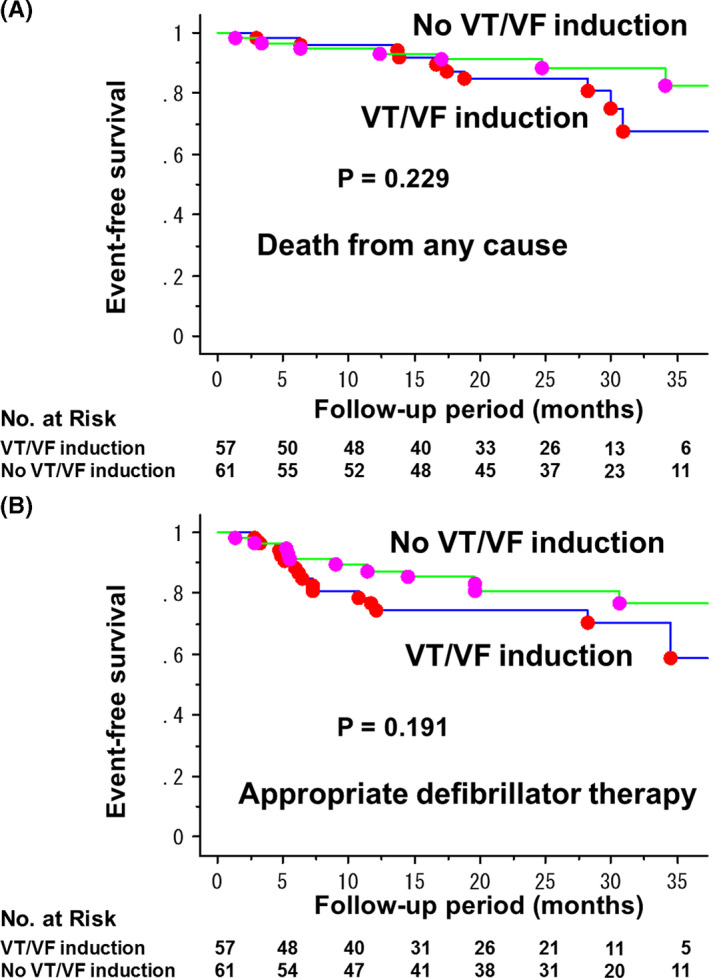
Electrophysiological study (EPS) with programmed ventricular stimulation had been performed before the device implant in 118 patients (15.8%, EPS group). During the mean follow-up of 21 ± 12 months, the rate of freedom from any death and appropriate defibrillator therapy was not significantly different between EPS group (n = 118) and No EPS group (n = 628). NYHA class II-IV, and QRS duration were negatively associated with performing EPS. Among patients in the EPS group, the rate of ventricular tachycardia (VT)/ventricular fibrillation (VF) induction was 48%. The inducibility was not a predictor of appropriate defibrillator therapy, whereas BNP ≧535 pg/mL and no use of amiodarone were significantly associated with a risk of the appropriate therapy.
EPS for induction of VT/VF had been performed in about 16% of patients with reduced LVEF before primary prevention ICD/CRT-D implantation. Elevated BNP levels and no use of amiodarone, but not inducibility of VT/VF, appeared to be associated with appropriate defibrillator therapy in these populations.
本研究旨在阐明程控心室刺激在无持续性室性心律失常且左心室射血分数(LVEF)降低的患者中的现状及作用。
分析日本心脏器械治疗注册研究(JCDTR)的随访数据,该研究纳入了2011年1月至2015年8月期间接受初次植入式心律转复除颤器(ICD)或心脏再同步化治疗除颤器(CRT-D)植入的746例LVEF≤35%且无持续性室性心律失常病史的患者。
118例患者(15.8%,电生理研究组)在器械植入前进行了程控心室刺激的电生理研究(EPS)。在平均21±12个月的随访期间,电生理研究组(n = 118)和非电生理研究组(n = 628)在任何死亡和合适的除颤治疗方面的无事件生存率无显著差异。纽约心脏协会(NYHA)心功能分级II-IV级和QRS时限与进行电生理研究呈负相关。在电生理研究组患者中,室性心动过速(VT)/室性颤动(VF)诱发率为48%。诱发率不是合适的除颤治疗的预测指标,而脑钠肽(BNP)≥535 pg/mL和未使用胺碘酮与合适治疗的风险显著相关。
在一级预防ICD/CRT-D植入前,约16%的LVEF降低患者进行了诱发VT/VF的电生理研究。在这些人群中,BNP水平升高和未使用胺碘酮似乎与合适的除颤治疗相关,而不是VT/VF的诱发率。