From the Department of Surgery, University of Alberta, Edmonton, Alta. (Goplen, Beaupre, Churchill); the School of Public Health, University of Alberta, Edmonton, Alta. (Randell, Jones, Voaklander); the Department of Physical Therapy, University of Alberta, Edmonton, Alta. (Randell, Jones, Beaupre); and the Alberta Bone and Joint Institute, Calgary, Alta. (Kang).
Can J Surg. 2021 Mar 5;64(2):E135-E143. doi: 10.1503/cjs.007319.
Up to 40% of patients are receiving opioids at the time of total knee arthroplasty (TKA) in the United States despite evidence suggesting opioids are ineffective for pain associated with arthritis and have substantial risks. Our primary objective was to determine whether preoperative opioid users had worse knee pain and physical function outcomes 12 months after TKA than patients who were opioid-naive preoperatively; our secondary objective was to determine the prevalence of opioid use before and after TKA in Alberta, Canada.
In this retrospective analysis of population-based data, we identified adult patients who underwent TKA between 2013 and 2015 in Alberta. We used multivariable linear regression to examine the association between preoperative opioid use and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain and physical function scores 12 months after TKA, adjusting for potentially confounding variables.
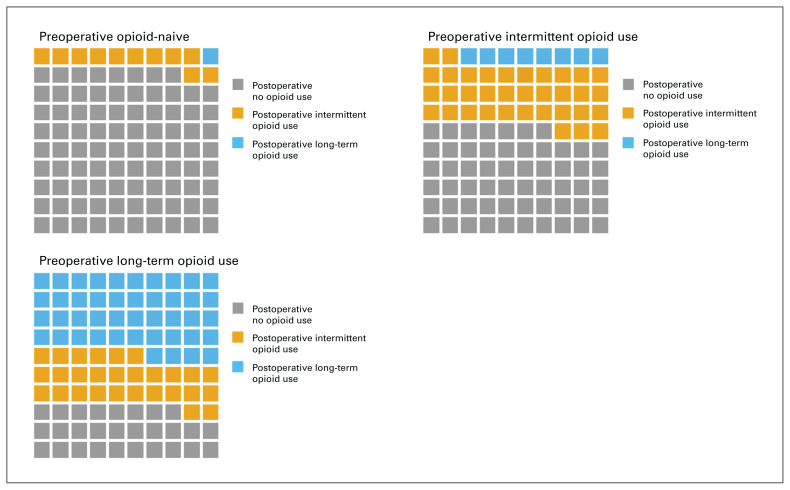
Of the 1907 patients, 592 (31.0%) had at least 1 opioid dispensed before TKA, and 124 (6.5%) were classified as long-term opioid users. Long-term opioid users had worse adjusted WOMAC pain and physical function scores 12 months after TKA than patients who were opioid-naive preoperatively (pain score β = 7.7, 95% confidence interval [CI] 4.0 to 11.6; physical function score β = 7.8, 95% CI 4.0 to 11.6; p < 0.001 for both). The majority (89 ([71.8%]) of patients who were long-term opioid users preoperatively were dispensed opioids 180-360 days after TKA, compared to 158 (12.0%) patients who were opioid-naive preoperatively.
A substantial number of patients were dispensed opioids before and after TKA, and patients who received opioids preoperatively had worse adjusted pain and functional outcome scores 12 months after TKA than patients who were opioidnaive preoperatively. These results suggest that patients prescribed opioids preoperatively should be counselled judiciously regarding expected outcomes after TKA.
尽管有证据表明阿片类药物对关节炎相关疼痛无效且存在较大风险,但在美国,多达 40%的接受全膝关节置换术(TKA)的患者正在接受阿片类药物治疗。我们的主要目标是确定术前使用阿片类药物的患者在 TKA 后 12 个月的膝关节疼痛和身体功能结果是否比术前未使用阿片类药物的患者更差;我们的次要目标是确定在加拿大艾伯塔省,TKA 前后阿片类药物使用的患病率。
在这项基于人群数据的回顾性分析中,我们确定了 2013 年至 2015 年期间在艾伯塔省接受 TKA 的成年患者。我们使用多变量线性回归来检查术前使用阿片类药物与 Western Ontario 和 McMaster Universities Osteoarthritis Index(WOMAC)疼痛和身体功能评分之间的关联,调整了潜在的混杂变量。
在 1907 名患者中,592 名(31.0%)在 TKA 前至少开具了 1 种阿片类药物,124 名(6.5%)被归类为长期阿片类药物使用者。长期阿片类药物使用者在 TKA 后 12 个月的调整 WOMAC 疼痛和身体功能评分比术前未使用阿片类药物的患者更差(疼痛评分β=7.7,95%置信区间 [CI] 4.0 至 11.6;身体功能评分β=7.8,95%CI 4.0 至 11.6;p<0.001)。与术前未使用阿片类药物的患者相比,术前长期使用阿片类药物的患者中有 89 例(71.8%)在 TKA 后 180-360 天内开具了阿片类药物,而术前未使用阿片类药物的患者有 158 例(12.0%)。
大量患者在 TKA 前后开具了阿片类药物,术前使用阿片类药物的患者在 TKA 后 12 个月的调整疼痛和功能结果评分比术前未使用阿片类药物的患者更差。这些结果表明,术前开具阿片类药物的患者应谨慎告知 TKA 后预期的结果。