Rehmani Razia, Segan Scott, Maddika Srikanth Reddy, Lei Yadanar Win, Broka Andrea
Chief of Neuroradiology & Musculoskeletal Imaging, Department of Radiology, SBH Health System, NY, USA.
Chief of Neurology SBH Health System, Department of Neurology, SBH Health System, NY, USA.
Brain Behav Immun Health. 2021 May;13:100238. doi: 10.1016/j.bbih.2021.100238. Epub 2021 Mar 3.
Coronavirus Disease 2019 (COVID-19) initially thought to be confined to the respiratory system only, is now known to be a multisystem disease. It is critical to be aware of and timely recognize neurological and neuroradiological manifestations affecting patients with COVID-19, to minimize morbidity and mortality of affected patients.
We performed a retrospective chart review of patients admitted to our Level 1 trauma and stroke center during the peak of the COVID-19 outbreak in New York from March 1st to May 30, 2020, with a positive test for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) who presented mainly with neurological findings and had acute radiological brain changes on Computed Tomography (CT) scan. Patients with known chronic neurological disease processes were excluded from the study. We obtained and reviewed demographics, complete blood count, metabolic panel, D-dimer, inflammatory markers such as erythrocyte sedimentation rate (ESR), C reactive protein (CRP), imaging, and patient's hospital course. We reviewed the current literature on neuroimaging, pathophysiology, and their clinical correlations on COVID-19. This case series study was approved by our institutional review board.
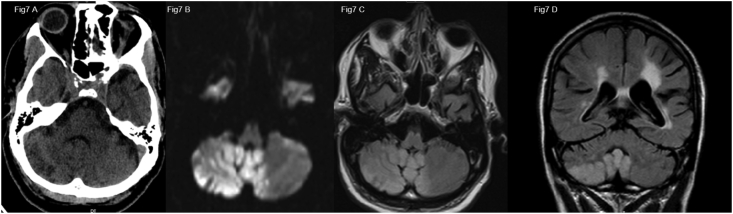
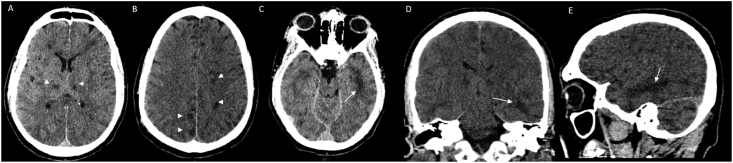
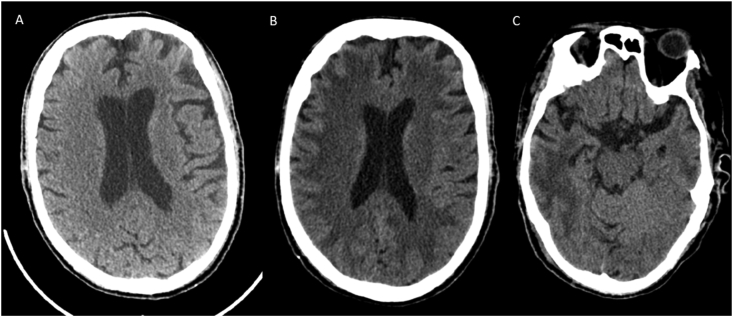
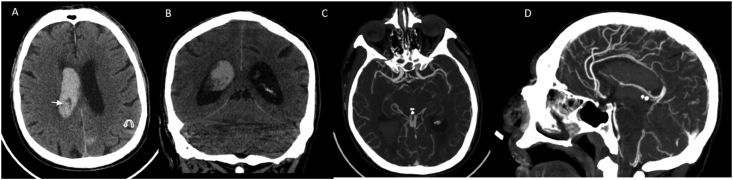
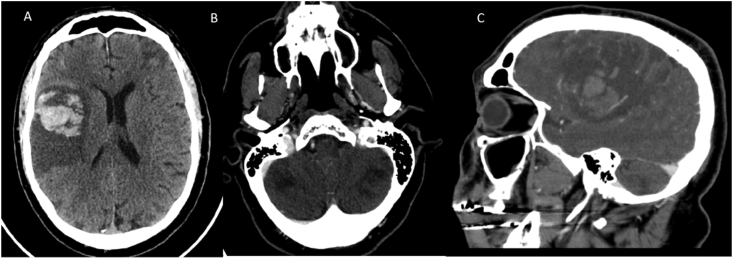
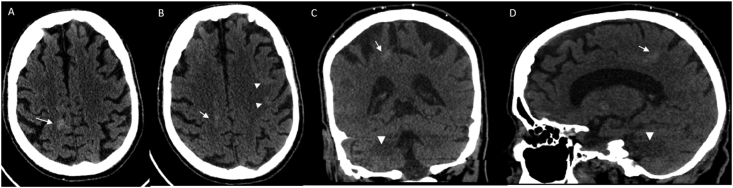
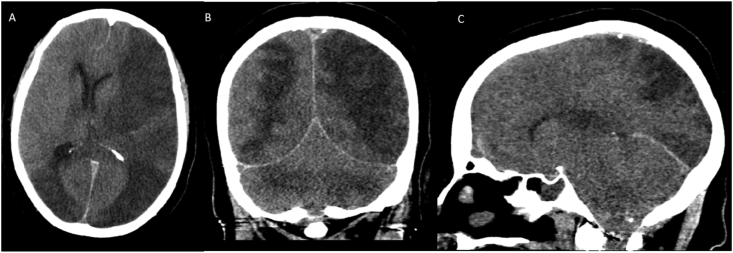
A total of 16 patients were selected for our case series. The most common neuroimaging features on CT, were territorial to multifocal ischemic infarcts, followed by a combination of ischemia and acute white matter encephalopathic changes, followed by temporal lobe predominant focal or more generalized encephalopathy with both confluent and non-confluent patterns, isolated cortical or more extensive intracranial hemorrhages and some combination of ischemia or hemorrhage and white matter changes. All our patients had severe acute respiratory distress syndrome (ARDS), most of them had elevated inflammatory markers, and D dimer.
COVID-19 infection is a multi-organ disease, which can manifest as rapidly progressive neurological disease beyond the more common pulmonary presentation. Early recognition of various neurological findings and neuroimaging patterns in these patients will enable timely diagnosis and rapid treatment to reduce morbidity and mortality. Our retrospective study is limited due to small non-representative sample size, strict selection criteria likely underestimating the true extent of neurological manifestations of COVID-19, mono-modality imaging technique limited to predominantly CT scans and lack of CSF analysis in all except one patient. Multi-institutional, multi-modality, largescale studies are needed with radio-pathological correlation to better understand the complete spectrum of neurologic presentations in COVID-19 patients and study the causal relationship between SARS-CoV-2 and CNS disease process.
2019冠状病毒病(COVID-19)最初被认为仅局限于呼吸系统,现在已知是一种多系统疾病。了解并及时识别影响COVID-19患者的神经和神经放射学表现,对于将受影响患者的发病率和死亡率降至最低至关重要。
我们对2020年3月1日至5月30日纽约COVID-19疫情高峰期入住我们一级创伤和卒中中心的患者进行了回顾性病历审查,这些患者严重急性呼吸综合征冠状病毒2(SARS-CoV-2)检测呈阳性,主要表现为神经学症状,且计算机断层扫描(CT)显示脑部有急性放射学改变。已知患有慢性神经疾病的患者被排除在研究之外。我们获取并审查了人口统计学数据、全血细胞计数、代谢指标、D-二聚体、炎症标志物如红细胞沉降率(ESR)、C反应蛋白(CRP)、影像学检查以及患者的住院病程。我们回顾了当前关于COVID-19神经影像学、病理生理学及其临床相关性的文献。本病例系列研究已获得我们机构审查委员会的批准。
我们的病例系列共纳入16例患者。CT上最常见的神经影像学特征是从区域性到多灶性缺血性梗死,其次是缺血与急性白质脑病改变并存,然后是以颞叶为主的局灶性或更广泛的脑病,有融合和非融合模式,孤立的皮质或更广泛的颅内出血,以及缺血或出血与白质改变的某种组合。我们所有患者均患有严重急性呼吸窘迫综合征(ARDS),大多数患者炎症标志物和D-二聚体升高。
COVID-19感染是一种多器官疾病,除了更常见的肺部表现外,还可表现为快速进展的神经疾病。早期识别这些患者的各种神经学表现和神经影像学模式将有助于及时诊断和快速治疗,以降低发病率和死亡率。我们的回顾性研究存在局限性,因为样本量小且不具代表性,严格的选择标准可能低估了COVID-19神经学表现的真实程度,单一的影像学技术主要限于CT扫描,且除一名患者外所有患者均未进行脑脊液分析。需要开展多机构、多模式、大规模研究,并进行放射病理学相关性分析,以更好地了解COVID-19患者神经学表现的全貌,并研究SARS-CoV-2与中枢神经系统疾病过程之间的因果关系。