Dreborg Sten, Kim Harold
Department of Child and Adolescent Allergology, Women's and Children's Health, University of Uppsala, 751 85, Uppsala, Sweden.
Department of Medicine, Western University, London, Canada.
Allergy Asthma Clin Immunol. 2021 Mar 8;17(1):25. doi: 10.1186/s13223-021-00511-y.
For a century, epinephrine has been the drug of choice for acute treatment of systemic allergic reactions/anaphylaxis. For 40 years, autoinjectors have been used for the treatment of anaphylaxis. Over the last 20 years, intramuscular epinephrine injected into the thigh has been recommended for optimal effect.
To review the literature on pharmacokinetics of epinephrine autoinjectors.
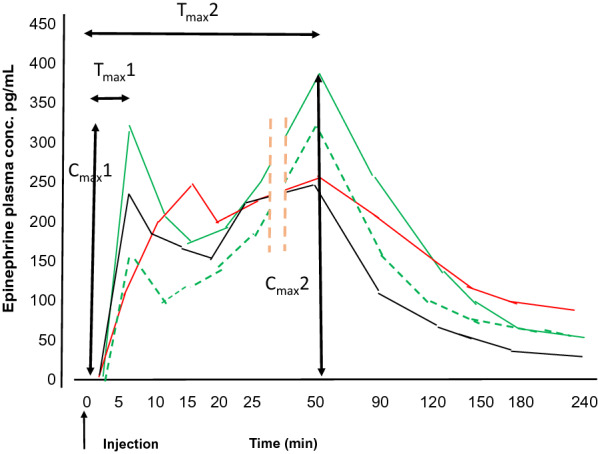
Six studies assessing epinephrine autoinjector pharmacokinetics were identified. The studies, all on healthy volunteers, were completed by Simons, Edwards, Duvauchelle, Worm and Turner over the span of 2 decades. Simons et al. published two small studies that suggested that intramuscular injection was superior to subcutaneous injection. These findings were partially supported by Duvauchelle. Duvauchelle showed a proportional increase in C and AUC when increasing the dose from 0.3 to 0.5 mg epinephrine intramuscularly. Turner confirmed these findings. Simons, Edwards and Duvauchelle documented the impact of epinephrine on heart rate and blood pressure. Turner confirmed a dose-dependent increase in heart rate, cardiac output and stroke volume. Based on limited data, confirmed intramuscular injections appeared to lead to faster C. Two discernable C were identified in most of the studies. We identified similarities and discrepancies in a number of variables in the aforementioned studies.
Intramuscular injection with higher doses of epinephrine appears to lead to a higher C. There is a dose dependent increase in plasma concentration and AUC. Most investigators found two C with T 5-10 min and 30-50 min, respectively. There is a need for conclusive trials to evaluate the differences between intramuscular and subcutaneous injections with the epinephrine delivery site confirmed with ultrasound.
一个世纪以来,肾上腺素一直是全身过敏反应/过敏性休克急性治疗的首选药物。40年来,自动注射器一直用于治疗过敏性休克。在过去20年中,推荐将肾上腺素注射到大腿肌肉中以获得最佳效果。
回顾肾上腺素自动注射器药代动力学的相关文献。
确定了六项评估肾上腺素自动注射器药代动力学的研究。这些研究均针对健康志愿者,由西蒙斯、爱德华兹、迪瓦舍尔、沃姆和特纳在20年的时间里完成。西蒙斯等人发表了两项小型研究,表明肌肉注射优于皮下注射。迪瓦舍尔的研究部分支持了这些发现。迪瓦舍尔发现,将肾上腺素肌肉注射剂量从0.3毫克增加到0.5毫克时,血药浓度峰值(C)和药时曲线下面积(AUC)成比例增加。特纳证实了这些发现。西蒙斯、爱德华兹和迪瓦舍尔记录了肾上腺素对心率和血压的影响。特纳证实心率、心输出量和每搏输出量呈剂量依赖性增加。基于有限的数据,证实肌肉注射似乎能使血药浓度峰值出现得更快。在大多数研究中发现了两个可辨别的血药浓度峰值。我们在上述研究的一些变量中发现了异同。
高剂量肾上腺素肌肉注射似乎能导致更高的血药浓度峰值。血浆浓度和药时曲线下面积呈剂量依赖性增加。大多数研究者发现有两个血药浓度峰值,其达峰时间分别为5 - 10分钟和30 - 50分钟。需要进行确定性试验,以评估肌肉注射和皮下注射之间的差异,并通过超声确认肾上腺素的给药部位。