London School of Hygiene and Tropical Medicine, London, UK.
Clinical Effectiveness Unit, The Royal College of Surgeons of England, London, UK.
Colorectal Dis. 2021 Jul;23(7):1733-1744. doi: 10.1111/codi.15622. Epub 2021 Apr 8.
The object of this work was to study how National Health Service hospitals in England and Wales aimed to maintain effective and safe colorectal cancer (CRC) services during the first peak of the COVID-19 pandemic (April 2020).
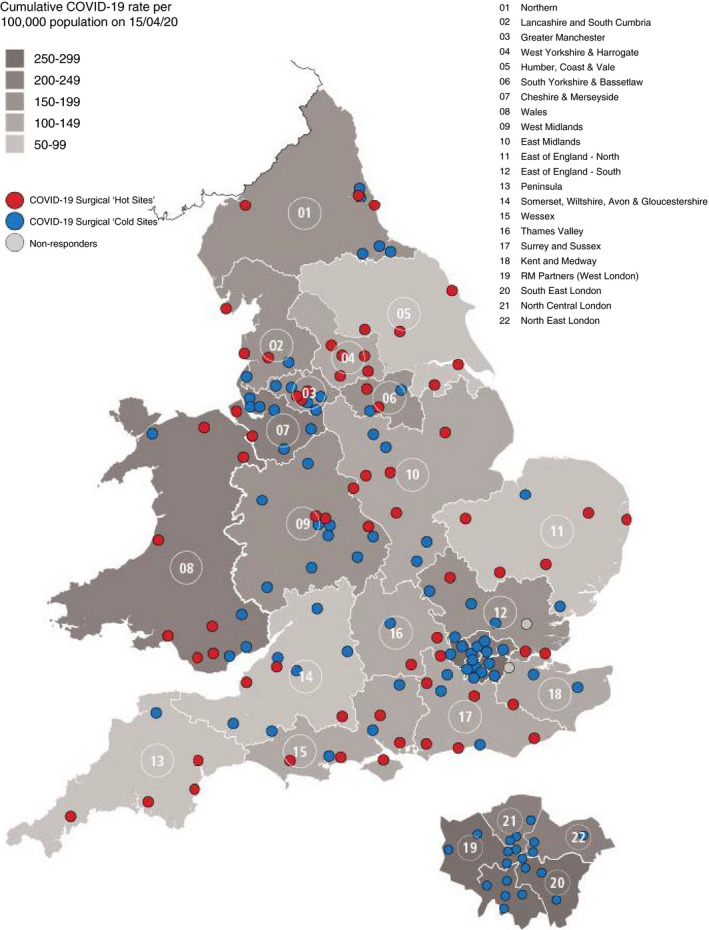
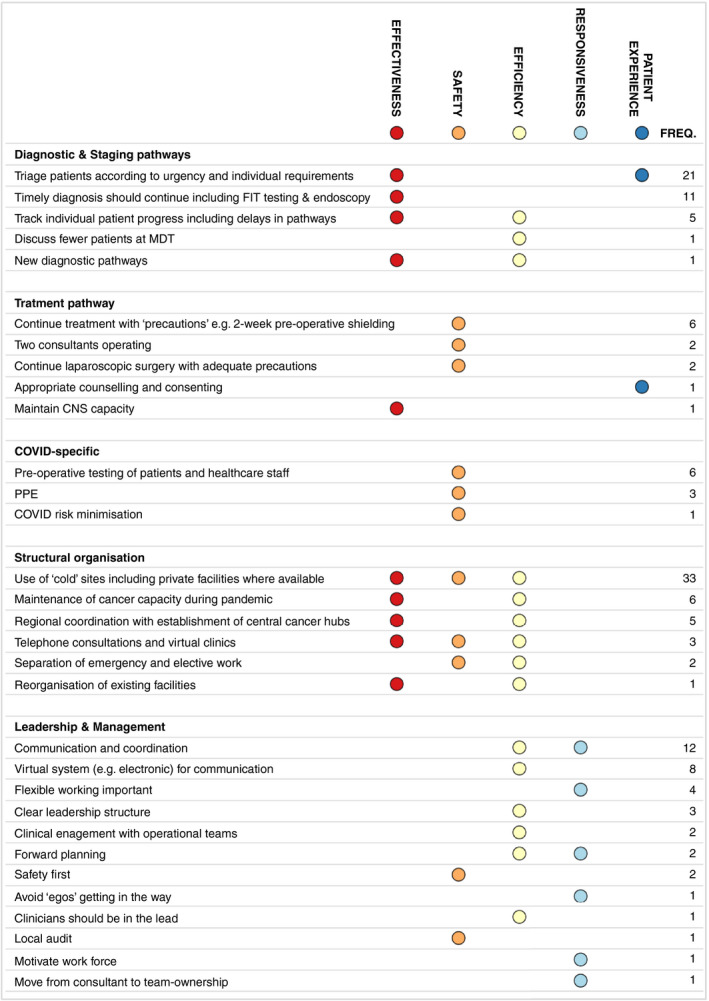
A national survey was performed among all 148 hospitals providing CRC services. Information was collected about changes in referrals, diagnostic, staging and therapeutic procedures, as well as whether there was access to a 'cold site' (a hospital facility free of COVID-19). Clinicians in each hospital were also asked to give the 'single most important lesson learned' about keeping services safe and effective.
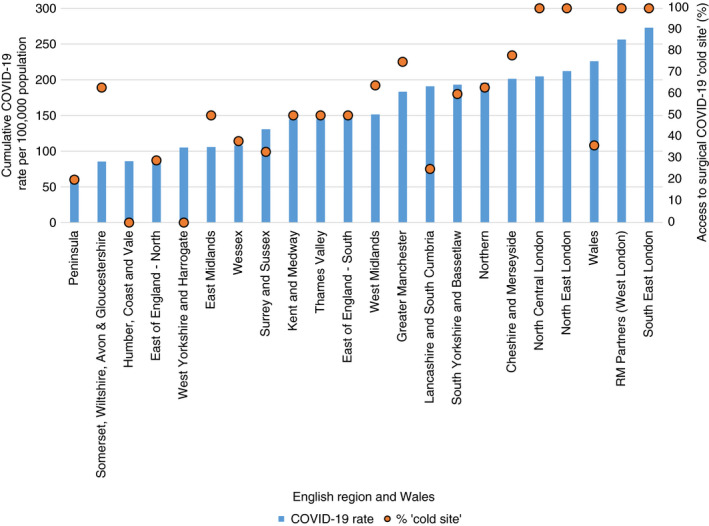
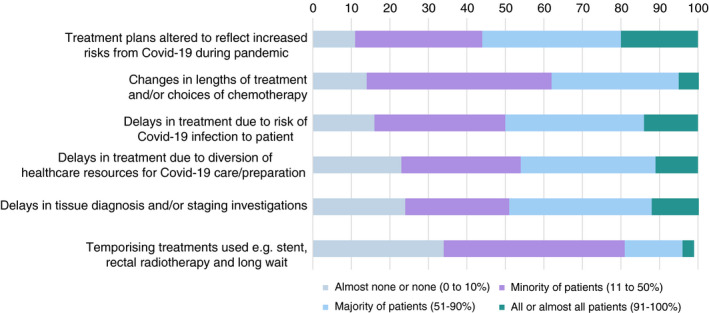
Full responses were received from 123 (83%) hospitals, and information about 'cold sites' was available for 146 (99%). Eighty hospitals (54%) had access to a 'cold site' and this was increased in regions with higher COVID-19 infection rates (p <0.001). Of the 123 responding hospitals, 105 (85%) indicated that referrals of patients with suspected CRC had dropped by at least 30%, and 69 (56%) indicated that treatment plans were altered in at least 50% of CRC patients. However, 'cold site' availability protected the capacity for diagnostic colonoscopy (p = 0.013) and CRC resection (p = 0.010). Many 'lessons learned' highlighted the importance of adequate structural service organization, often mentioning 'cold sites' and regional coordination as examples, good communication and triage of patients based on clinical urgency.
Access to 'cold sites', as well as regional coordination, clear communication and strong leadership, were found to be pivotal in maintaining capacity for diagnosis and treatment of CRC during the COVID-19 surge.
本研究旨在探讨英格兰和威尔士的国民保健制度(NHS)医院如何在 COVID-19 大流行的第一个高峰(2020 年 4 月)期间维持有效的结直肠癌(CRC)服务。
对提供 CRC 服务的 148 家医院进行了全国性调查。收集了有关转诊、诊断、分期和治疗程序的变化信息,以及是否可以使用“冷站点”(没有 COVID-19 的医院设施)。还要求每家医院的临床医生提供有关保持服务安全有效的“最重要的经验教训”。
收到了 123 家(83%)医院的完整回复,146 家(99%)医院提供了“冷站点”的信息。80 家(54%)医院可以使用“冷站点”,且在 COVID-19 感染率较高的地区增加(p<0.001)。在 123 家做出回应的医院中,有 105 家(85%)表示疑似 CRC 患者的转诊量至少下降了 30%,有 69 家(56%)表示至少有 50%的 CRC 患者改变了治疗计划。然而,“冷站点”的可用性保护了诊断性结肠镜检查(p=0.013)和 CRC 切除术(p=0.010)的容量。许多“经验教训”强调了充分的服务组织结构的重要性,经常提到“冷站点”和区域协调作为例子,还强调了良好的沟通和基于临床紧急程度的患者分诊。
在 COVID-19 疫情高峰期,获得“冷站点”以及区域协调、明确的沟通和强有力的领导,对于维持 CRC 的诊断和治疗能力至关重要。